


Complaint to the NHS regarding the Cass Review
NHS England Case Reference 2410-2154543 - NC NHSE:0223488

14th October 2024
Dear NHS complaints team/Gender dysphoria team,
I would like to make a complaint regarding the “Independent Review of gender identity services for children and young people”, the “Cass Review”.
I would like to make two points in this complaint:
1) The Cass Review omitted “lived experiences” and research regarding autogynephilia.
2) The Cass Review’s 11th recommendation, to commission “regional services” across the country, is treating the symptom, and not the cause of the problem, namely that children, primarily girls, are misdiagnosing themselves with a “mismatched” “gender identity”.
I would consider a successful outcome of my complaint to be the following:
a) The NHS to issue advice to charities, organisations, schools and non-governmental organisation to remove all content regarding cross-sex identification (content related to “gender identity”, “non-binary”, “gender incongruence” etc.) and advise for these organisations to signpost parents and children to the NHS instead.
b) The NHS include a paragraph on the phenomenon of “autogynephilia” on its web page on “gender dysphoria”: https://www.nhs.uk/conditions/gender-dysphoria/
The Cass Review omitted “lived experiences” and research regarding autogynephilia.
Omission of lived experiences
My personal narrative “lived experience” of cross-sex identification and autogynephilia, which was part of paragraphs 2-4 of my Charity Commission complaint regarding multiple charities was confirmed as received by the Cass Review on the 21st April 2022.
My lived experience will be the same as for most adolescent boys, who suddenly announce that they are women.1
Adolescent boys who suddenly announce that they are women and want hormones, e.g. who are autogynephilic, are still children, and will be represented in those presenting with gender dysphoria to child and adolescent services.
Accordingly, the Cass Review should have included my lived experience, and discussion of the phenomenon of autogynephilia in the review under “Understanding the patient cohort”.
I include my narrative again here:
At the onset-of puberty, at the age of 13-14, I found that I was not only attracted to women, but also to the concept of myself as woman. I felt like a “lesbian inside a man’s body”.2
As an adolescent trying to understand my developing sexuality, one of the most confusing things trying to understand was my apparent bisexuality, despite having no attraction to men in real life.

I entered what I felt into an online search engine, and discovered the research by the Canadian clinical psychiatrist Ray Blanchard, who is currently an adjunct professor at the University of Toronto.
I found that Blanchard described the phenomena that I felt, to an uncanny accuracy, and called the phenomenon as a whole “autogynephilia”,3 which is Greek for “attraction to the concept of oneself as a woman”, which Blanchard concluded was one of two reasons behind gender identity disturbances in males:
“Gender identity disturbance in males is always accompanied by one of two erotic anomalies. All gender dysphoric males who are not sexually oriented toward men are instead sexually oriented toward the thought or image of themselves as women. … the writer would prefer to replace it with the term autogynephilia (“love of oneself as a woman”)”.
Blanchard further accurately described my confusing sexuality as “pseudobisexuality”:
“….bisexual gender dysphorics’ interest in male sexual partners is mediated by a particularly strong desire to have their physical attractiveness as women validated by others. This “bisexual” behavior need not reflect an equal erotic attraction to the male and female physiques (and would perhaps be better characterized as pseudobisexuality)”.4
Autogynephilia is not just words on the page, but an atypical sexuality, a paraphilia, and you cannot really understand it, if you do not experience it.
I found out through a Freedom of Information request, that I was by no means the only individual who shared their lived experience regarding autogynephilia with the Cass Review, which were marked “strictly confidentially [sic]”, “where relevant anonymously”, “not to be shared”.
Again, the Cass Review should have discussed my lived experience, and these other lived experiences, under “Understanding the patient cohort”.
Omission of research regarding autogynephilia
I sent my “Trans memo” to the Cass Review, which illustrates the research around autogynephilia, and the way in which it can be observed in public life under the label of “gender identity”. This was confirmed as received by the review on the 1st December 2023.
The research regarding autogynephilia should have been mentioned under “Understanding the patient cohort”.
This research is not only important for autogynephilic gender dysphorics, and their parents, but also important to the parents of children with early-onset gender dysphoria, who should know to discount the narratives of the late-onset autogynephilic gender dysphoria of male adolescent and adults, as not applying to their son.
If the parents of children with early-onset gender dysphoria confuse what their son is experiencing with narratives of late-onset gender dysphoria (adolescents, and adults), then they will be left with a false impression that what their son is experiencing is unlikely to resolve, despite the DSM-5 saying that in most cases, what their son is feeling will resolve at the onset of puberty, when they are also likely to find that they are same-sex attracted (DSM-5 p. 455).
There is no justification for the Cass Review not to cover the extensive research regarding autogynephilia, when the Cass Review mentions “non-binary” 31 times, despite “non-binary” not appearing in the DSM-5 at all, connected to gender dysphoria or otherwise, and having no comparable body of academic research.
Furthermore, autogynephilia seems to be a phenomenon that the medical profession seems to be generally aware of. For example, I sent my “Trans memo” to a consultant child and adolescent psychiatrist, who replied:
“Thanks for your interesting Substack. I believe your piece helpfully highlights about a number of key points… The issue is not just a simple one of “it’s just how we are”, but is a very complex web of issues most likely. I do suspect most are social phenomenon, and as you say the role of AGP [autogynephilia]”.
This response further indicates that there was no justification for the Cass Review to omit the phenomenon of autogynephilia from the review.
The Cass Review’s 11th recommendation, to commission “regional services” across the country, is treating the symptom, and not the cause of the problem, namely that children, primarily girls, are misdiagnosing themselves with a “mismatched” “gender identity”.
If the Cass Review had covered all the causes of cross-sex identification, namely autogynephilia, a recommendation to ban the misleading “mismatched” “gender identity” narrative from being targeted at children would have been inescapable.
This is the misleading narrative that repurposes the term “gender identity” in the DSM-5, and uses it to suggest that cross-sex identification is supposedly a matter of a “mismatched” “gender identity”, a reformulation of the well-known “feminine essence” narrative, which suggests that “transsexuals are in “some literal sense and not just in a figurative sense, women inside men’s bodies” (transsexuals being historically mostly male-to-female).56 This has more in common with a belief system than an evidence base, as it appeals to some essential quality that exists outside our sexed bodies.
This misleading narrative is usually accompanied with the false statement that this matter has nothing to do with sexual orientation or sexuality;7 the complete opposite of what is conveyed by the DSM-5:
The DSM-5 says that identifying as a different “gender” which the DSM-5 takes as “man”, or “woman” to one’s sex (male, female) is directly connected to atypical sexual orientation or sexuality: homosexuality or autogynephilia.
In the case of what the DSM-5 calls “early-onset gender dysphoria”, which occurs in early childhood, it says that in most cases such dysphoria will cease, and that these children are are likely to grow up same-sex attracted (DSM-5 p. 455).
In the case of what the DSM-5 calls “late-onset gender dysphoria”, experienced by adolescents and adults, usually males, it says that individuals “frequently engage in transvestic behavior with sexual excitement” (DSM-5 p. 456). The DSM-5 says that in males, autogynephilia, a paraphilia, increases the likelihood of gender dysphoria (DSM-5 p. 456).
The idea that a “mismatched” “gender identity” or “essence” itself causes cross-sex identification does not appear in the DSM-5.
I sent the Cass Review my complaint to the Charity Commission, that covered the way many charities were targeting this misleading “mismatched” “gender identity” “essence” narrative at children, and that this should be stopped, as it is causing a social contagion.
This social contagion is happening primarily amongst girls (illustrated below, and on page 24 of the Cass Review), who are misdiagnosing themselves as having a “mismatched” “gender identity” (below), despite fulfilling none of the actual diagnostic pathways as featured in the DSM-5.
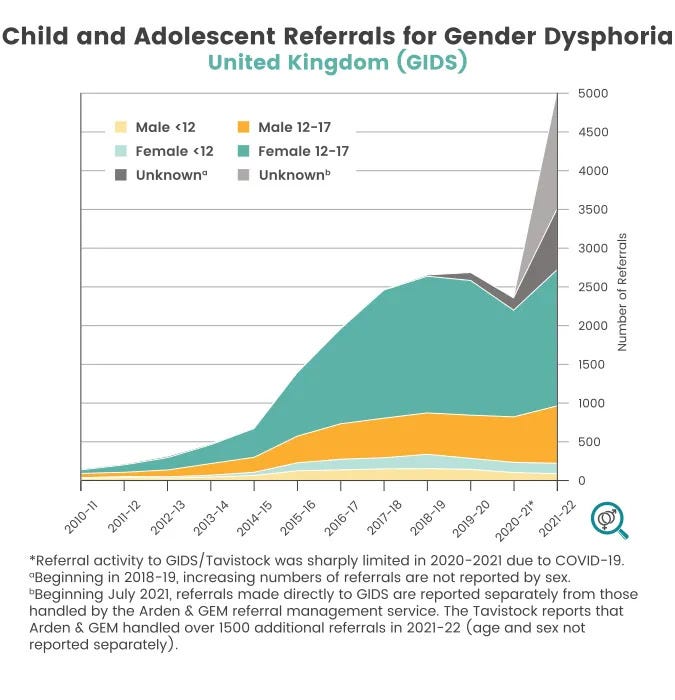
These girls and young women are in most cases not homosexual, and likely all do not have a paraphilia: their cross-sex identification is the result of a social contagion, from having been targeted with the misleading “mismatched” “gender identity” “essence” narrative. The Cass Review confirmed this complaint was received on the 21st April 2022.
I repeated this concern in the “Trans memo”, which the Cass Review received on the 1st December 2023 which additionally demonstrated how the “mismatched” “gender identity” “essence” is misleading, with illustrations of primary research. The Cass Review also confirmed it knew, on the 12th February 2024, about the republication of this memo in part by the organisation Genspect.
The memo further drew attention to the fact that it is primarily girls, a group that has historically always been vulnerable to social contagions, who are misdiagnosing themselves with a “mismatched” “gender identity”.
When there are clear diagnostic pathways to gender dysphoria, which are connected to atypical sexuality, namely, homosexuality (in which case gender dysphoria usually resolves at the onset of puberty) or autogynephilia (which only affects a few males), it is misleading to teach children that everyone has a “gender identity” which for some people can “mismatch”. The confusion that this narrative is creating is represented in statistics, as primarily girls and young women misdiagnose themselves with a psychological condition of gender dysphoria, despite not fulfilling the actual diagnostic pathways as described in the DSM-5.
Furthermore, when one knows about the actual causes of cross-sex identification, as they appear in the DSM-5, it becomes apparent that nothing about this topic is appropriate to teach indiscriminately to children. This was, accordingly, one of my desired complaint outcomes in my complaint regarding multiple charities to the Charity Commission: that nothing regarding cross-sex identification should be being taught to children, and that this matter instead by handled on a case-by-case basis.
If the Cass Review had covered the causes of cross-sex identification as they appear in the DSM-5, namely, homosexuality or autogynephilia, a recommendation to ban the “mismatched” “gender identity” “essence” narrative from being targeted at children would have been inescapable, as being something patently misleading.
This was the correct recommendation that was recently made for schools by the Department of Education, who incidentally, also received by “Trans memo”:
“Schools should not teach about the broader concept of gender identity. Gender identity is a highly contested and complex subject. It is a sense a person may have of their own gender, whether male, female or a number of other categories. This may or may not be the same as their biological sex. Many people do not consider that they or others have a separate gender identity.”8
The Cass Review’s 11th recommendation, that there should just be more clinics to deal with the psychological harm that is being created by the misleading “mismatched” “gender identity” “essence” narrative, is treating the symptom of this social contagion, and not the cause.
This is not good use of NHS resources. It is also unjust, for parents, primarily of girls, and the girls themselves, to have to go through suffering, as they misdiagnose themselves with a psychological condition, that they were never going to suffer from in the first place.
As a man with autogynephilia, who has known about autogynephilia since he was an adolescent boy, I see what is happening is wrong. Children should not be being told that everyone has a “gender identity”, that for some people can be “mismatched”, as it is not the truth about cross-sex identification, and is causing harm.
It is relevant for this complaint, that after the Cass Review was published, I followed up my memo by having an article published by the charity HealthSense, a charity that campaigns for science and integrity in healthcare, which covers the issues I raise in this complaint, showing that others in the medical profession share my same concerns.
Yours,
Orlando.
20th November 2024
Dear Orlando Woolf,
Thank you for reaching out to NHS England and taking the time to raise your concerns about the Independent Cass Review.
Your comments and feedback have been passed onto the Gender Dysphoria/Specialised commissioning service and they have been noted. Please below response:
I am sorry that you are not happy with the process, however the Cass Review was an independent review, with its own process in its entirety. This process was not run by NHS England, it set terms of reference, which the review designed its own methodology to answer.
Following the Cass Review, NHS England will be working with Providers through the National Provider Collaborative to coordinate the development of evidence-based information and resources for young people, parents and carers.
The Cass Review called for professional bodies to come together to provide leadership and guidance on the clinical management of this population and the Charity Commission has already advised charities in the UK (through its report on the investigation of Mermaids) on how they should ensure that public facing information is consistent with the findings of the Cass Review.
We thank you for your feedback.
Yours sincerely
[…]
20th November 2024
Dear […],
Please could you forward my reply below:
Does NHS England acknowledge that the Cass Review omitted the lived experience of myself and others regarding autogynephilia?
Will NHS England include a paragraph on autogynephilia on its page on “Gender dysphoria”?
Despite the Charity Commission's investigation, Mermaids continues to mislead children and parents with the narrative that that matters of cross-sex identification are somehow a matter of a “mismatched” “gender identity” “essence”. I cover how this is misleading in paragraph 22 of my complaint.
I have made a complaint to Mermaids regarding this, however it is clear that they will not stop with this misleading narrative, unless the NHS’s page on “gender dysphoria” were to cover the actual causes of gender dysphoria, as they appear in the DSM-5, which would include autogynephilia.
Furthermore, the Charity Commission continues to allow Stonewall and GIRES to to make unevidenced claims regarding puberty blockers, despite it now being 6 months after the Cass Review, and despite having received two complaints:
https://transpolicy.substack.com/p/charity-commission-complaint-regarding-c75
https://transpolicy.substack.com/p/charity-commission-complaint-regarding-d2a
The Charity Commission is not fulfilling their role as a regulator.
Below is my exchange with Mermaids from after the Charity Commission’s investigation:
26th October 2024
Dear Mermaids,
I would like to make a complaint regarding your content related to "gender dysphoria" which is addressed at families. [1]
I personally have experience of what today is called "gender dysphoria". Some years ago, at the onset of puberty, I was confused regarding my sex. I had the feeling that I was a "lesbian trapped inside a man's body". I was also confused regarding my sexuality. In fantasy, I imagined myself as a woman with a man, however, I had no attracted to men in real life.
I entered what I felt online, and came across the research by Ray Blanchard, who accurately described what I felt as "autogynephilia". I have found that this phenomenon has caused varying intensities of gender dysphoria throughout my life.
I therefore find your content misleading, which says that somehow cross-sex identification arises out of a "difference between their gender identity and the gender or sex they were assigned at birth", as it's not telling families the full truth about this issue.
[1] https://mermaidsuk.org.uk/families/
Yours,
Orlando
28th October 2024
Dear Orlando,
I am responding to your email as a complaint, and in line with our complaints procedure.
I have reviewed your complaint and the content of the website section you reference. The information contained there is brief and is not intended to be a full explanation of gender dysphoria, its causes or treatment.
We have based our information on that provided by the NHS which you can find here Gender dysphoria - NHS which states "Gender dysphoria is a term that describes a sense of unease that a person may have because of a mismatch between their biological sex and their gender identity".
As noted on the page, we do not give medical advice and would signpost to the NHS for specific medical advice or treatment.
I hope that answers your complaint and the rationale.
Regards,
Sandie
Director of Service Delivery
27th November 2024
Dear Orlando Woolf
Thank you for your further correspondence.
We are reviewing your correspondence and will be in touch again in due course.
Kind regards
16th December 2024
Dear Orlando Woolf
Thank you for your email.
I apologise for the delay in responding to your concerns, however the team are still reviewing your correspondence.
Thank you for patience on the matter.
Kind regards
6th January 2025
Dear Orlando Woolf
Thank you for your further correspondence.
After further review of your concerns regarding the Cass Review, the NHS England Gender Dysphoria/Specialised commissioning service have no further comment to add.
Our content team for the NHS website has added: The NHS website is currently reviewing its content on gender dysphoria to ensure it better meets the needs of people looking at the NHS website for this information. This work is still in progress and at this time we are unable to specify what the timeframe for this review would be and what the content will look like.
Your feedback is important to us, and we appreciate your time in raising this to us.
Kind regards
6th January 2024
Please could you escalate my complaint.
The NHS refusing to address the points raised in my complaint is not good enough.
I again repeat my questions:
Does NHS England acknowledge that the Cass Review omitted the lived experience of myself and others regarding autogynephilia?
Will NHS England include a paragraph on autogynephilia on its page on "Gender dysphoria"?
These are simple questions. The DSM-5 says autogynephilia increases the likelihood of gender dysphoria. (p. 703). The NHS now knows that the Cass Review received accounts from individuals speaking about autogynephilia, including myself. Freedom of Information shows that the Cass Review's mailbox had 44 emails in it about autogynephilia, some marked “strictly confidentially”, “where relevant anonymously”, “not to be shared”. [1] Autogynephilia is very easy to recognise. [2]
I am reading right now the "lessons to be learnt" to the contaminated blood scandal. One of these lessons is "Candour is essential in the relationship between clinicians and patients. Both patients in accepting treatment, and clinicians in advising on it, are badly affected by its absence." [3]
The NHS is not acting with candour over this issue. It should be unremarkable to say that "Yes, we will be covering all the causes of gender dysphoria, including autogynephilia, on our page on "Gender dysphoria"".
What is remarkable, is that NHS England want to start a puberty blocker clinical trial, yet appears unwilling to talk with candour about the causes of gender dysphoria. If the NHS wants to put children on a puberty blocker clinical trial, and does not tell parents the full story about this issue, including autogynephilia, then parents cannot give informed consent, as they are not being informed regarding the nature of gender dysphoria.
Parents should know that the experiences of late-onset gender dysphorics with autogynephilia, like me, are of no relevance to children with early-onset gender dysphoria, and that there are drastically different outcomes: early-onset gender dysphoria in the majority of cases will resolve by itself if left alone (DSM-5 p. 455). It is deeply wrong to continue with the narrative, as the NHS's current page on "Gender dysphoria" does, that everything is explained by a "mismatched gender identity".
[1] https://www.healthsense-uk.org/publications/newsletter/newsletter-128/434-128-letter.html
[2] https://transpolicy.substack.com/p/how-to-recognise-autogynephilia
[3] https://www.mills-reeve.com/publications/infected-blood-inquiry-lessons-to-be-learned/
Yours,
Orlando
7th January 2025
Dear Orlando Woolf,
I am sorry to hear you are dissatisfied with the responses provided. We believe we have responded appropriately to the questions you have raised and have no further comments to make.
If you remain dissatisfied, and you would like to take the matter further, you can refer the matter to the Parliamentary and Health Service Ombudsman (PHSO) and they will be able to confirm if they can take the matter further. The PHSO is an independent service which is free for everyone to use.
Any further correspondence received on this matter will be filed but not responded to.
We appreciate the time you have taken in raising your concerns to us.
Yours sincerely
7th January 2025
Dear […],
This is an occasion when deferring to some other authority is not good enough. NHS England is showing that it has learned no lessons from the contaminated blood scandal.
NHS England is pushing for a puberty blocker clinical trial. This is the time when it needs to answer my questions. If NHS England cannot answer these questions candidly, it has no business trying to implement a puberty blocker trial:
Does NHS England acknowledge that the Cass Review omitted the lived experience of myself and others regarding autogynephilia?
Will NHS England include a paragraph on autogynephilia on its page on "Gender dysphoria"?
NHS England need to be able to talk candidly and truthfully about gender dysphoria, as it has implications for informed consent. I have been complaining about this issue since 2022. [1] The excuse for years has been that NHS England has been waiting for the Cass Review. Now NHS England offers no excuse, and simply refuses to address my complaint.
It's not good enough. and neither is trying to defer responsibility regarding this issue to members of parliament, who are not clinicians.
[1] https://transpolicy.substack.com/p/complaint-to-the-nhs-regarding-page
Yours,
Orlando
11th February 2025
Dear Orlando,
Please find attached NHS England’s final response to your National Complaint case 2410-2154543.
There are over 200 accounts similar to mine in the book Men Trapped in Men’s Bodies (Springer, 2013) which I also cited in the Charity Commission complaint that I sent to the Cass Review. https://annelawrence.com/book/
This is listed as a diagnostic feature in the DSM-5, for “late-onset gender dysphoria (adolescence, adulthood)” “After gender transition, many self-identify as lesbian.” DSM-5 p. 456.
Blanchard, R. “The Classification and labelling of nonhomosexual gender dysphorias”. Archives of Sexual Behavior 18(4) 315-334 p. 323. September 1989. p. 323
Blanchard, R. “The Concept of Autogynephilia and the Typology of Male Gender Dysphoria”. The Journal of Nervous and Mental Disease. October 1989. p. 622
Blanchard, R. “Deconstructing the Feminine Essence Narrative”. Archives of Sexual Behavior 2008;37:434-438
I have previously made a complaint to the NHS regarding this narrative and the “Gender Identity Research and Education Society”

This was a substantive point in my complaint to the Charity Commission that I sent to the Cass Review:

“The department welcomes your research, and officials acknowledge the memo you have provided”. https://consult.education.gov.uk/rshe-team/review-of-the-rshe-statutory-guidance/supporting_documents/Draft%20RSE%20and%20Health%20Education%20statutory%20guidance.pdf