


Complaint to the Charity Commission regarding Fumble
CRM:0049126

Dear Charity Commission,
Complaint regarding Fumble (1188089)
Fumble has the charitable objects to “to advance the education of the public, particularly young people up to the age of 25, on the subject of sexual health, wellbeing and relationships in such ways as the trustees think fit”.
As the Charity Commission recently noted, “Charity law requires that the information provided by education charities, or those with an object to advance education, is accurate, evidence based and balanced.”1
I would like to make two points of complaint: first, that Fumble is signposting children and young people towards GenderGP, and second, that Fumble is not giving children and young people accurate and evidence-based information regarding what the DSM-5 calls “gender dysphoria”, encouraging self-misdiagnoses and self-harm.
I would consider a successful outcome to my complaint, for Fumble to stop signposting children to GenderGP, and for it to remove its content regarding gender dysphoria.
Fumble signposting children to GenderGP
In Fumble’s “Support and resources for trans+ young people” Fumble signposts children towards GenderGP.2
The NHS has issued a safety alert against GenderGP, warning GPs not to work with the organisation.3
GenderGP have come out strongly against the Cass Review’s conclusion,4 that puberty blockers have “unclear rationale” and “weak evidence” for their use.5
GenderGP’s website apparently allows circumvention of the now indefinite ban on puberty blockers issued by the Health Secretary under the Medicines Act 1968.6
Signposting children and young people towards GenderGP therefore poses both a risk of recommending a medical treatment that has unclear rationale for its use, and also leaving any purchaser at risk of committing a criminal offence under the Medicines Act 1968.
It is important that the GenderGP loophole is closed and the organisation not recommended, as the government notes:
“Closing legal routes to access the products may mean that those with this protected characteristic may turn to unregulated, black market sources of puberty blockers. However, this type of sale or supply is also prohibited under the emergency order and will constitute a criminal offence. These actions will protect children from starting a course of treatment which may be unsafe and harmful and for which the evidence base is weak.”7
Fumble does not provide accurate and evidence based information regarding what is called “gender dysphoria” in the DSM-5.
Vague symptoms presented out-of-context
Fumble omits information regarding the very specific diagnostic pathways that the DSM-5, (covered in paragraph 33 onwards below) and gives the impression that matters of a cross-sex identification are a matter of a “gender identity”, construed as a type of essence or feeling, “not aligning” with one’s sex,8 a vague description that encourages self-misdiagnoses.
Fumble further encourages symptoms of gender dysphoria, e.g. body dysmorphia, to be taken out of the context of gender dysphoria as described in the DSM-5 (below), encouraging children and young people, particularly girls and young women, with body dysmorphia, to misdiagnose themselves with gender dysphoria.
For example, a 16-year old girl who has the the common experience of body dysmorphia that has arisen out of unwanted sexual attraction, may misdiagnose herself with gender dysphoria, despite this not being the same as the body dysmorphia that has arisen out of what the DSM-5 calls “late-onset” gender dysphoria, which is described below:
“I’m a 28-year-old male who has experienced arousal from autogynephilia since the age of 12. I always thought I was weird, because I’ve never been effeminate. When I hit puberty, around age 12, I remember being aroused seeing girls growing boobs and also seeing my stepmother’s bras and panties in the laundry area. I remember being attracted to girls themselves but having extreme arousal over the thought of being a girl and growing boobies. I already fantasized about being a girl and having a vagina before the boob thing started. It’s hard to pinpoint when I realized I was highly aroused by this, but I believe it was when I saw some girls in my class at a play wearing leotards and tights or pantyhose at a school play. I wanted so bad to have a vagina and be free of my penis...”9
Fumble recommends that girls and young women can wear breast binders to “lessen feelings of dysphoria”.10 This is encouraging self-harm when gender dysphoria is self-misdiagnosed, which Fumble encourages through vague diagnostic criteria that does not represent gender dysphoria.
My example above, of a 16-year old girl misdiagnosing herself with gender dysphoria and receiving dangerous advice is not speculation. Many young women are now describing their misdiagnoses that have happened in this way, and have engaged in self harm that Fumble recommends. Charlie Bentley-Astor, a detransitioner who started to transition at the age of 13, describes this in interview:
“It began in my head. I began to view myself different, began to refer to myself differently. I gave myself a different name in my own head. Then I created a persona online that was a kind of aspirational self, and so the goal was to make my real self as much like the ideal self that I was online. That involved binding my breasts, first with sports bras, layering them up, then with bandages and baggy clothes, to try and cover what evidence was left after that, starving myself, trying to stop my body from developing more than it had… the whole experience for me was encapsulated for me in an instance when a man wolf-whistled at me. I must have been 11 or 12, and by then I had the smallest rumouring of female body developing… I didn’t understand that my developing would change my relationship to society… that was the most distressing thing about it.”11
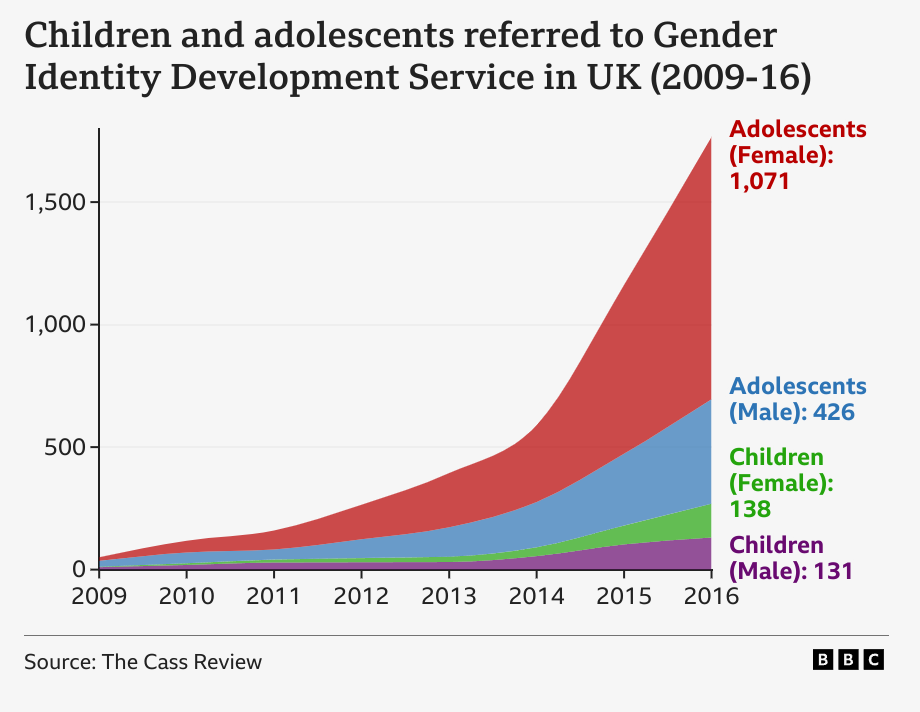
Girls and young women are a well-known cohort for suffering social contagions; misdiagnosing themselves with mental health conditions. This is also represented in statistics, as girls have been drastically over-represented in referrals to gender clinics (below).
Fumble encourages these misdiagnoses, by presenting symptoms of gender dysphoria out of their context in the very specific pathways (“early-onset” homosexual/“late-onset” autogynephilic) mentioned in the DSM-5, which I further cover in my complaint to Fumble (paragraph 33 onwards of this complaint).
“Transvestic behavior with sexual excitement” referred euphemistically as “gender euphoria”
In Fumble’s page “How to affirm your gender identity safely”,12 Fumble refers to “gender euphoria”. This is not a concept that appears in the DSM-5, connected to gender dysphoria or otherwise.
The DSM-5 says that, “Adolescents and adults with late-onset gender dysphoria frequently engage in transvestic behavior with sexual excitement.”13 Fumble appears naive to the fact that “gender euphoria” has been propagated as a euphemism to describe cross-dressing with sexual excitement.
This euphemism further encourages children, like Bentley-Astor, to misdiagnose their relief, or “euphoria”, at binding their their breasts, as gender dysphoria.
It can be further observed it the media, how “gender euphoria” is being used euphemistically to refer to the transvestic behavior with sexual excitement that characterises “late-onset” gender dysphoria:

“She [sic] vividly remembers the first time she explored that wardrobe, at the age of nine. Her mother was at work, her father asleep downstairs in his chair. Hannah crept into their bedroom and tentatively opened a drawer. She took out a silky nightgown and shrugged it on, feeling the instant, giddy rush of something she would later learn to call “gender euphoria”, though it was tempered by fear that someone would walk in.”
Fumble, and evidently others, like the Guardian, who misconstrue gender dysphoria as some mismatched “gender identity” essence that has “not align[ed]” with one’s sex (paragraph 12 of this complaint), appear to be unaware of how the DSM-5 actually describes gender dysphoria as being connected to atypical sexuality: homosexuality or autogynephilia.
Gender dysphoria is a rare condition
Gender dysphoria is a rare condition. The DSM-5 says that in the case of “early-onset” gender dysphoria, most cases will resolve themselves at the onset of puberty, where the individual also has a high likelihood of being homosexual. The DSM-5 says that in the case of “late-onset” gender dysphoria, this will be something only likely experienced by males, like me, with an unusual paraphilia; autogynephilia.
Historically, it has been autogynephilic transsexuals, with “late-onset” gender dysphoria, who were most representative of this condition. This would include historical figures like Lili Elbe, who was compelled to undergo dangerous treatments like vaginoplasty, as autogynephilia can create body dysmorphia similar to another paraphilia, apotemnophilia, which is the male paraphilia to amputate one’s limbs to resemble an amputee.
Women and girls therefore were never largely represented amongst those with gender dysphoria, Yet, today there are thousands of adolescent girls and young women presenting to “gender clinics” with gender dysphoria. I can only see that charities like Fumble are encouraging this to happen.
It is not in the public interest for Fumble to encourage children and young people to misdiagnose themselves with gender dysphoria, through omitting context to diagnostic criteria, or referring to diagnostic criteria through misleading euphemisms.
It is not in the public interest, and presents a demonstrable risk to vulnerable supposed beneficiaries, for Fumble to then encourage these children and young people, who are primarily girls and young women, to then engage in self-harm through breast binding.
12th December 2024
Dear Fumble,
I would like to make the complaint that your page on gender dysphoria, [1] which characterises it as “when someone feels a disconnection, sense of unease or distress from their gender identity not ‘aligning’ (according to cisnormativity) with their sex assigned at birth” is misleading as it does not represent the diagnostic description of gender dysphoria in the DSM-5.
Paragraph 33
The DSM-5 says that there are two types of gender dysphoria: what it calls “early-onset” and “late-onset”. [2] In the case of early-onset gender dysphoria, this is characterised as when a particularly masculine girl or feminine boy may identify as the opposite sex, which in most cases will desist at the onset of puberty, when they will find that they are same-sex attracted. [3]
In the case of “late-onset” gender dysphoria, this is characterised in males by “frequently engag[ing] in transvestic behavior with sexual excitement”. [4] The DSM-5 notes that a concept called autogynephilia (the “Sexual arousal of a natal male associated with the idea or image of being a woman” [5]) “increases the likelihood of gender dysphoria” amongst this cohort. [6]
In my case, I have what the DSM-5 calls “late-onset” gender dysphoria with autogynephilia.
It is therefore also evident, that the content that you link to “s3xtheorywithdee” which describes the “3 types of gender dysphoria” is also incorrect: there are only two-types of gender dysphoria in the DSM-5, and these are connected to atypical sexuality, namely homosexuality, or autogynephilia, as mentioned above.
The content “s3xtheorywithdee” furthermore is vague as to what it describes as gender dysphoria, e.g. “Body dysphoria is a sense of unease a person may experience when their gender identity doesn't align with their biological sex/body”.
It is easy to see how a child or adolescent may misdiagnose themselves with having “gender dyphoria” after reading such vague criteria, which are presented out-of-context from the two diagnostic pathways mentioned in the DSM-5.
For example, a heterosexual girl who is unhappy with her body may come to believe she has a “gender identity that doesn't align” with her sex, and misdiagnose herself with gender dysphoria, despite not fulfilling any of the diagnostic pathways in the DSM-5, being neither homosexual and certainly not autogynephilic.
Indeed, the drastic increase in girls presenting to “gender identity clinics” over the last ten years, which is primarily amongst adolescent girls, a cohort that is notorious for experiencing social contagions, suggests these self-misdiagnoses are happening very frequently.
The Cass Review mentions “diagnostic overshadowing” as having been a significant problem amongst clinicians, where "many of the children and young people presenting have complex needs, but once they are identified as having gender-related distress, other important healthcare issues that would normally be managed by local services can sometimes be overlooked." [7]
I would suggest that your content encourages this “diagnostic overshadowing”, but from the perspective of adolescent girls themselves, as they misdiagnose themselves with gender dysphoria using your vague criteria, which does not represent what is in the DSM-5.
Please could you remove or revise your content.
[1] https://fumble.org.uk/gender-dysphoria-experiences-youre-not-alone/
[2] DSM-5 p. 455
[3] DSM-5 p. 455
[4] DSM-5 p. 455
[5] DSM-5 p. 818
[6] DSM-5 p. 703
[7] Cass Review p. 17
Yours,
Orlando
17th December 2024
Thank you for reaching out. We have received and acknowledged your complaint.
Fumble aims to provide accurate information to its users and to deliver the best possible service to the organisations and individuals with which it works. Fumble's primary beneficiaries are young people in the UK and we take great care to ensure that the information we provide for these young people is correct and in line with UK public health guidelines.
In this instance, we are satisfied that the content referenced meets both our own rigorous quality standards and the recommended public health guidelines in the UK (specifically from the NHS and WHO).
All the best,
The Fumble team
23rd December
Dear Orlando Woolf FUMBLE : 1188089 C-151831-P8P0
Thank you for your online form submitted on 19 December.
We understand you are concerned about the charity and appreciate you sending us information. You have raised a concern that the charity may not be acting in accordance with updated NHS guidelines, specifically in relation to issues of gender identity and gender dysphoria. Our decision We have carefully reviewed all the information you sent us. From the information you have submitted, we can see that you have raised your concerns directly with the charity and received confirmation that the charity’s literature, website and guidance has been reviewed in light of relevant guidance and legislation.
Based on this, we are assured that appropriate action is already being taken to address these concerns. For this reason, we will not be contacting the charity about this issue. How we make our decisions When making our decisions, we consider the issue and look at the risk to anyone who comes into contact with the charity, along with the risk to the charity itself. It’s important that we consider the likely impact of our involvement, so we can make a fair and balanced decision about whether to act.
All decisions are made following the principles set out in the Charity Commission Regulatory and Risk Framework.
10th January 2025
Dear Orlando Woolf RE: RELATE (207314); FUMBLE (1188089)
I am writing in response to your email received on 12 December 2024 in which you raised concerns about the action the Charity Commission (‘the Commission’) took when dealing with your complaint about an article published on the website of Relate.
I understand that my colleague, Ms […], responded to you on 25 October 2024 regarding the same concerns in respect of information published on various charity websites. I have considered this correspondence along with the case records to inform my consideration of your most recent complaint. I have decided that it would be appropriate for me to consider your complaint about Relate in the same manner and as a continuance of the stage two response in October 2024.
I am also responding to your email of 23 December regarding your request for a stage two complaint review of our response to your concerns about Fumble 1188089
This is the final stage of our process, and our usual parameters is to determine Ms […] responses in respect of Relate and Fumble addressed the issues of your complaint; dealt with any shortfalls in our service; conveyed the outcome clearly; and was thorough and fair.
Your concerns: I have noted that you remain concerned with the Commission’s approach to the concerns you raised about the charities, Relate and Fumble, and you would like us to include consideration of your views regarding Stonewall Equality Ltd. Charity Commission
Relate
Our records show the Assessment Manager, […], reviewed your concerns about the information contained on the charity’s website, and decided it was appropriate to issue advice and guidance to the charity. Ms [...] notified you of this decision on 10 December 2024. In the letter, Ms […] informed you that it is not for the Commission to determine whether information issued and published by the charity is correct. Ms […] decided that the best way forward was to provide the trustees with regulatory advice and guidance about ensuring that they have regard to the findings, conclusions and recommendations of the Cass Review and ensuring that they have reviewed their charity’s literature, website and guidance in light of them.
I am satisfied that Ms […] response addressed your concerns raised about the charity. The decision to issue advice and guidance was fair and proportionate action to take. However, having reviewed, our case records it would have been helpful to have acknowledged that you remained concerned about Stonewall Equality Ltd and provided you with a response to this point. I am aware that we have previously provided Stonewall Equality Ltd with advice and guidance, and I can confirm that we will not be taking any further action at this stage.
Fumble
Our records show the Assessment Manager […] reviewed your concern that the charity may not be acting in accordance with updated NHS guidelines, specifically in relation to issues of gender identity and gender dysphoria. Based on the response to your complaint directly from the charity, we took the decision not to contact the charity as we were assured that the appropriate action is already being undertaken. I am satisfied that Ms […] response was a proportionate and fair response, to your concerns, and that it was appropriate for us not to contact the charity. I appreciate you taking the time to notify the Commission about your concerns in respect of the charities and that your concerns and your opinions on how others should communicate about the issues stem from your lived experience. It evident that you feel strongly about the matter as you continue complete complaints forms raising concerns about various charities regarding the information on their respective websites in relation to gender identity. Summary I am satisfied that the Commission has fully considered your concerns in respect of both Relate and Fumble.
I appreciate that you would like us to take further action, however our letter of 25th October outlined in detail the Commission’s functions. This correspondence also addressed our actions regarding Stonewall Equality Ltd. I will not rehearse this content in this letter.
I have identified that it would been helpful to say in our previous letter that we have previously provided advice and guidance to Stonewall Equality Ltd, and we would not be taking any further action. I apologise for this missed opportunity. This concludes my consideration of your complaint at stage two of the Commission’s complaint process. If you remain dissatisfied with the service you have received, you can ask your MP, to approach the Parliamentary and Health Service Ombudsman (PHSO). The PHSO considers certain complaints about the service provided by a range of bodies including the Commission. Further information is available here – Complaints procedure - The Charity Commission - GOV.UK (www.gov.uk) Yours sincerely,
10th January 2025
Dear Charity Commission,
Please could you send […] the following message that I have sent Fumble this morning. Please could I confirm that […] is fine that Fumble silently removing their link to GenderGP poses no risk.
Dear Fumble,
I saw that you removed your link to GenderGP.
Did you know how many children and young people have accessed GenderGP through this link?
Do you think that you should post a message, warning children and young people, that if they had followed your advice up until December 18th 2024 -- that they should be careful to desist contact with GenderGP?
If they do not know to desist contact with GenderGP, children and young people could put themselves at risk of criminal prosecution and receiving supposed medical treatments that lack medical rationale and evidence for their use.
Yours,
Orlando
10th January 2025
Dear Charity Commission,
Following on from my previous message, I completely reject your characterisation of this matter: "It [sic] evident that you feel strongly about the matter as you continue complete complaints forms raising concerns".
I keep on raising complaints, as as noted in paragraph 36 of my complaint CRM:0049403, the Charity Commission has a history of failure in addressing false medical health claims.
The Charity Commission's history of failure regarding false medical health claims, combined with false information about the nature of cross-sex identification, is now proving to be badly harming children, primarily girls, who are misdiagnosing themselves as having the "gender identity" of the opposite sex, and being recommended to bind their chests by charities such as Fumble.
The Charity Commission says that it is "not qualified to make judgments about evidence in health care" [2] however, the Charity Commission is not even willing to stop charities making false medical claims, despite clear guidance from the NHS in the form of the Cass Review.
I made my complaint regarding puberty blockers in April 2024, [1] however Stonewall's misleading content remains. You have not said how many times you have contacted Stonewall. Is it just once?
Furthermore, the Charity Commission expects complaints to continually be made: "We learned that the Commission does not undertake to monitor compliance with regulatory advice, and that if we still have concerns we should make further complaints." [2]
Yours,
Orlando
[1] https://transpolicy.substack.com/p/charity-commission-complaint-regarding-c75
[2] https://www.healthsense-uk.org/publications/newsletter/newsletter-123/362-123-rose.html
6th February 2025
Dear Charity Commission,
Please could you escalate my complaint regarding Stonewall, GIRES and Fumble (CRM:0049125) to your CEO, David Holdsworth.
The Charity Commission writes "A charity can raise people’s awareness of an issue to build support for a campaign, provided this furthers the charity’s purposes. Engagement in campaigning is a means by which many charities work to further their purposes."
If Stonewall and GIRES want to campaign for a clinical trial regarding puberty blockers, then they are welcome to. However making false claims regarding medical treatments does not come under campaigning; that comes under making false claims regarding medical treatments.
The Charity Commission has now received very clear advice in this area from the NHS in the form of the Cass Review, as mentioned in my complaint. I think it can now be argued, that the Charity Commission itself has taken a political stance on a medical issue, in its choice not to issue a regulatory alert regarding charities that are continue to make false claims regarding puberty blockers. This isn't acceptable.
The Charity Commission writes, "We have not identified any evidence that Stonewall or GIRES are encouraging or enabling children to obtain puberty blockers".
I have provided evidence in my complaint CRM:0049125. To make false claims regarding the benefits of a medical treatment, is to encourage the public, and children, to seek that treatment out. This is only a web-search away.
The Charity Commission writes, "We can see that Fumble has reviewed the content on the website and taken action. It is not the role of the Commission to become involved in how the trustees handled the changes made to their website. This is a decision for the trustees to make."
The Charity Commission is not following its Risk and Regulatory Framework.
If a supermarket sells a product that is harmful for consumption, then it will issue a product recall. A charity should similarly issue a statement to discontinue using a service, that it had previously recommended, if this service now puts its users at risk of receiving a criminal record, and receiving a supposed medical treatment, which the government says poses an "acute risk" to the "health and wellbeing" of children.
As it stands, the parents and children who had previously received advice from Fumble to use GenderGP, are being left completely in the dark regarding this issue. Now, both Fumble and the Charity Commission show a complete lack of concern regarding the risk this poses to supposed beneficiaries.
Yours,
Orlando
Anne Lawrence Men Trapped in Men’s Bodies: Narratives of Autogynephilic Transsexualism (Springer: 2013).
Charlie Bentley Astor in conversation with Andrew Gold. “Woke Doctors lied: My Trans Mistake is permanent.”
DSM-5 p. 456