


Charity Commission complaint regarding the Royal College of General Practitioners


27th May 2025
Dear Royal College of General Practitioners,
Please cascade the points of my complaint to the other Royal Colleges. You can refer to this easy-to-understand article by Bailey & Blanchard:
I have tried to raise this issue with the Royal College of Physicians, with the contact point of Dr […].
The "gender identity" scandal is a medical scandal, like the contaminated blood scandal, and the thalidomide scandal. I have always known this to be true, based on the fact that I am self-aware that I have autogynephilia. If you had autogynephilia, you would be sending this message yourselves.
Furthermore, your own GPs know what is happening is a scandal:
Internal activists and external lobby groups have a stronghold within organisations such as the Royal College of GPs (RCGP). This activism has no doubt enabled the indoctrination of the NHS by an ideology, and as a result the NHS has discarded its ethical framework in the guise of caring, or being kind. However, being kind necessitates striving to practice evidence based medicine, striving to do no harm, and striving to practice the art of medicine, which requires exploration, not affirmation.
What is happening is horrific medical malpractice: "Father's letter begging top surgeon to cancel trans operation on 'depressive' 20-year-old: 'Please don't remove my daughter's breasts ...in just one day you'll ruin her life for ever".
Whenever I read this headline, I feel a pit in my stomach, as as I know that I have autogynephilia, I know that this man's daughter is suffering from a social mental health contagion. Your medical profession is doing this to thousands of young women.
This issue should have ended with the Cass Review, which I wrote to several times. However the Cass Review omitted any discussion of autogynephilia.
I subsequently made a Freedom of Information request on the Cass Review, and found around 44 other men also shared their "lived experience" of autogynephilia with the Cass Review, which were similarly ignored.
The man who has one of the most publicised cases of medical malpractice, Ritchie Herron, has now also written about his subsequent awareness that autogynephilia was at the root of his cross-sex identification. These surgeries are now happening to two men a day. It is impossible that there is informed consent, because the medical profession refuses to discuss autogynephilia.
Instead, the medical profession is operating on a false belief, that there are a class of "transgender" people, even children, who infallibly know they have the "gender identity" "incongruent gender" i.e. "essence" of the opposite sex or something else entirely, like "non-binary". As the medical profession is trusted to undertake surgery and prescribe drugs, this false belief means that harm is occurring without limit.
Please hold an EGM to create content that properly describes "gender dysphoria", with a paragraph about autogynephilia, and to discuss the medical malpractice that is happening. You should recommend for there to be a stop on prescriptions and surgeries in this field of so-called medicine, which is operating without any underlying logic or indication.
Yours,
Orlando Woolf
23rd May 2025
Dear Orlando,
Thank you for your and I hope you are well.
I can confirm receipt of your email, which is being dealt with internally.
Kind regards,
[snip]
[Office of the President]
21st May 2025
Dear Royal College of General Practitioners,
Please find attached [at the top of this Substack] the complaint I would like to raise with the Charity Commission regarding the Royal College of General Practitioners.
I am sending my complaint to you as the email that you have given on the Charity Commission's website does not work.
Please could you let me know if there is any alternative way to resolve the issues I have raised in the complaint.
[snip]
Yours,
Orlando Woolf
20th May 2025
Dear Charity Commission,
I would like to make the complaint that the Royal College of General Practitioners (RCGP) is not fulfilling their charitable object to “to encourage, foster and maintain the highest possible standards in general medical practice.”
I have asked several times since 2024, for the RCGP to update its content related to “transgender care” to represent the diagnostic pathways and descriptions of “gender dysphoria” as they appear in the DSM-5.
I can see that by not doing so, that the RCGP is contributing to the current mental health social contagion (illustrated on page 9) occurring primarily amongst adolescent girls and young women, who are misdiagnosing themselves using misleading and incorrect descriptions of “transgender” and “gender dysphoria” and who are then being physically harmed by a negligent medical profession, e.g. “The mothers left distraught after the NHS removed their daughters’ healthy breasts because the girls said they were transgender” Daily Mail, Sanchez Manning, 27th February 2025).
I have included my correspondence with the RCGP below.
Yours,
Orlando Woolf
16th May 2025 9:33 AM
Dear Ruth Ellenby,
Thank you for your response. However it is not an appropriate response given the issues that I raise.
This is because the medical scandal that Dr. Ray Blanchard [1], and others, could see of vulnerable “…troubled adolescents, especially adolescent girls. [Being put] at risk for unnecessary, disfiguring, and unhealthy medical interventions”, is now being implemented by your medical profession in great volume, e.g.: “The mothers left distraught after the NHS removed their daughters’ healthy breasts because the girls said they were transgender” (Daily Mail, Sanchez Manning, 27th February 2025).
The grief caused by later regret for these surgeries is now accordingly also being documented. [2] An appropriate response, would be for you to escalate this issue, with view of updating the RCGP’s content to provide General Practitioners with the most basic knowledge of what “gender dysphoria” is, as described in the DSM-5, and how it is likely to resolve.
This would also be a small, yet significant, action that the RCGP can take, to contribute towards ending the medical scandal that is happening in your wider medical profession, of primarily adolescent girls and young women misdiagnosing themselves with a condition that they do not have, and then receiving unnecessary, unhealthy and disfiguring medical treatments.
I know this, as I experience the actual condition of “late-onset gender dysphoria”. I have attached an illustrated PDF [further down this Substack] of a more comprehensive version of my complaint, [page 5 onwards] which also covers the conflicts of interest that likely exist in your “patient groups” and “key stakeholders” in not wanting to discuss matters of cross-sex identification honestly, which has resulted in your content not covering the most basic details about “gender dysphoria”, as they appear in the DSM-5.
If you are not able to handle my complaint, please could you escalate my complaint.
[1] Blanchard served on the DSM-4 subcommittee for “gender identity disorders”.
[2] “Breastfeeding grief after chest masculinisation mastectomy and detransition: A case report with lessons about unanticipated harm” Karleen D Gribble, Susan Bewley, Hannah G Dahlen. Front Glob Womens Health. 2023 Feb 3:4:1073053.
Yours,
Orlando Woolf.
16th May 2025 9:39 AM
Dear Orlando,
I’m sorry to hear you do not feel the response is adequate.
I’m copying back in our member services team who will be able to advise you on routes to escalate your complaint should you wish to.
Best wishes,
Ruth
Head of Policy | Policy, Research and Campaigns
16th May 2025
Good morning Orlando
I hope you are well.
As we have been unable to resolve your Formal Complaint to your satisfaction, you now will have to escalate your complaint externally.
You have further recourse via external organisations depending on the nature of the complaint - for example the Charity Commission, HMRC or Information Commissioners Office.
Kind regards,
Annaliese
Senior Member Service Manager
Royal College of General Practitioners
16th May 2025
Dear Annaliese, Ruth,
I have documented how I have already raised my concerns with the relevant external body, namely the Charity Commission on paragraph 55 [page 14] of my complaint [further down this Substack] to you, and how nothing was done.
Specifically, the Charity Commission said that they were not medical professionals, so were not capable of assessing my complaint. The Charity Commission responded: “The Commission has considered the issues raised and our assessment is that we lack the expertise and knowledge of complicated psychological and medical issues connected to gender identities to be able to form a definitive view on the issues you have raised.”
You are suggesting to do something that is demonstrably inappropriate. It is the content of the RCGP that I am complaining about, and you are the medical professionals who are capable of evaluating my complaint.
Accordingly, please could you escalate my complaint to the President, or CEO of the RCGP, or the appropriate next authority above yourself in the RCGP.
Yours,
Orlando
19th May 2025
Dear Ruth Ellenby,
As you would have seen from being copied into my messages with Annaliese, the suggestion that I ask the Charity Commission to address my concerns with the RCGP is inappropriate, given that the Charity Commission has already told me that it lacks the ability to assess medical matters.
Annaliese’s other suggestion, that I take up my complaint with the RCGP with HMRC, arguably shows that the RCGP is not taking the well-substantiated concerns I raise in my complaint seriously.
These concerns include conflict of interest (paragraphs 22 [page 7] and 28 [page 9]), medical malpractice (paragraph 57 [page 14]), and child abuse (paragraphs 25 [page 8] and 37 [page 10]).
The RCGP recently noted that there is an issue of medical health professionals not taking seriously the healthcare of women, [1] so this would be a good opportunity for the RCGP to take more time in investigating the example I gave of a woman receiving an unnecessary double mastectomy, and how this can be prevented.
The RCGP’s role in stopping this malpractice, at the very least, is for it to update its content regarding “gender dysphoria” for General Practitioners, so that the content actually covers the basic information and pathways that appear in the DSM-5. If you are not able to address my concerns, please could you escalate them to the next person of authority in the RCGP.
[1] https://www.rcgp.org.uk/gp-frontline/spring-2025-news-womens-health-hubs
Yours,
Orlando Woolf
19th May 2025
Dear Orlando,
Annaliese has advised on the College’s complaints policy which we are following on this matter.
I’m afraid I will not be able to engage further or reply to any further emails on this.
Best wishes,
Ruth
Ruth Ellenby
Head of Policy | Policy, Research and Campaigns
16th May 2025
Dear Ruth Ellenby, Head of Policy, Royal College of General Practitioners,
I would like to make the complaint that your content “Transgender care” poses a risk to patients, as it does not inform general practitioners regarding the basic information of the pathways behind “gender dysphoria” in the DSM-5, and how they are likely to resolve.
For example, I am a man with what the DSM-5 calls “late-onset gender dysphoria”, which starts at the onset of puberty (DSM-5 p. 455) connected to “autogynephilia” (“Sexual arousal of a natal male associated with the idea or image of being a woman. DSM-5 p. 818).
General practitioners should know that this has nothing to do with children with “early-onset gender dysphoria”, which starts before puberty, (DSM-5 p. 455-6) and is characterised as when a particularly masculine girl or feminine boy may identify as the opposite sex, which in most cases will desist at the onset of puberty, when they will find that they homosexual (DSM-5 p. 455).
Given the case of parents with a remarkably feminine boy, parents and general practitioners should know that the “early-onset gender dysphoria” that their son is experiencing has nothing to do with the “late-onset gender dysphoria” that I experience.
If they confuse what their son is experiencing with what I experience, they will be left with the false impression that what their son is experiencing is unlikely to resolve.
The fact that your content omits these pathways misleads general practitioners into believing that cross-sex identification is all explained by there supposedly being a class of people, even children, who have some sort of mismatched “essence”, or as the RCGP writes “incongruent gender”, of the opposite sex.
This is much different from what is conveyed by the DSM-5, that shows that cross-sex identification is a matter of atypical sexuality / sexual orientation: namely, either autogynephilia or homosexuality, and something that most children will grow out of.
The false belief, that there are a class of people, even children, who have some “mismatched” or “incongruent” “gender”, is now pervasive in the medical profession, and is resulting in medical malpractice, as it is the false basis under which primarily girls and young women, who have misdiagnosed themselves as having a “mismatched gender identity”, or now an “incongruent gender”, are receiving unnecessary, unhealthy, and disfiguring medical interventions.
I would consider a successful outcome of this complaint to be for the RCGP to cover the very basic information regarding “gender dysphoria” as it appears in the DSM-5. This would provide Gender Practitioners with the actual information they need to know, and contribute to ending what is a wider medical malpractice in your medical profession.
Background to “gender dysphoria”
The latest edition of the Diagnostic and Statistical Manual of Mental Disorders 5th Edition (DSM-5) says that “gender dysphoria… refers to the distress that may accompany the incongruence between one's experienced or expressed gender and one’s assigned gender” (DSM-5 p. 451).
The DSM-5 uses the word “sex” to refer to the “to the biological indicators of male and female” and uses the word “gender” to “denote the public (and usually legally recognized) lived role as boy or girl, man or woman” (DSM-5 p. 451).
An illustration of this framework could be that if a male is “assigned” a “gender” of a “boy”, and then “man”, but instead identifies as a the “gender” of a “girl” and then “woman”, then this male experiences “gender dysphoria”.
The DSM-5 says that there are two “broad trajectories” of gender dysphoria, which it calls “early-onset” and “late-onset” (DSM-5 p. 455).
Early-onset gender dysphoria
In the case of “early-onset gender dysphoria”, this is characterised as when a particularly masculine girl or feminine boy may identify as the opposite sex, which in most cases will desist at the onset of puberty, when they will find that they homosexual (DSM-5 p. 455). The previous DSM-4 manual noted that “In child clinic samples, there are approximately five boys for each girl referred with this disorder” (DSM-4 p. 535).
Late-onset gender dysphoria
In the case of “late-onset gender dysphoria” (adolescence, adulthood), starting “around puberty or much later in life”, this is characterised in males by “frequently engag[ing] in transvestic behavior with sexual excitement”. These males are otherwise heterosexual: “a substantial percentage of adult males with late-onset gender dysphoria cohabit with or are married to natal females” (DSM-5 p. 456). After gender transition, many self-identify as lesbian” (DSM-5 p. 456).
The DSM-5 says that a phenomenon called “autogynephilia”, (the “Sexual arousal of a natal male associated with the idea or image of being a woman”, DSM-5 p. 818), “increases the likelihood of gender dysphoria in men with transvestic disorder” (DSM-5 p. 703).
I am aware of these diagnostic descriptions, as I have what the DSM-5 calls “late-onset gender dysphoria” with autogynephilia. I found that I experienced autogynephilia, when at the onset of puberty, aged around 13-14, I searched online and found a synopsis of Dr. Ray Blanchard’s clinical descriptions of autogynephilia. “Autogynephilia” is the word that Blanchard coined to describe what he observed.
Inadequate consultation process
The RCGP writes “The statement was developed in consultation with a wide range of RCGP members, patient groups and key stakeholder organisations. I’m afraid we are not in a position to further discuss it or any changes to it at this point, but I would like to thank you again for your careful consideration of it.”
However the RCGP appears unaware of the fact that “patient groups” and “key stakeholder organisations” have conflicts of interest in not wanting to discuss the causes and pathways of “gender dysphoria” candidly and accurately.
The Gender Identity Research and Education Society
The organisation the “Gender Identity Research and Education Society” (GIRES), which has advised the RCGP in the past regarding this matter, refuses to cover autogynephilia in its content, and misleadingly suggests that matters of cross-sex identification have nothing to do with sexuality / sexual orientation i.e. the complete opposite to what is conveyed by the DSM-5.
I made a complaint in 2022 to GIRES regarding this, and Cat Burton, chair of trustees closed my complaint (paragraph 49 CRM:0467599) after I was at first promised a “full and comprehensive response”.
As Cat Burton’s personal narrative of “gender dysphoria” is similar to my own, it appears that he also has “late-onset gender dysphoria”, connected to autogynephilia:

“It was daunting contemplating transitioning, I’d buried all my gender issues when I was 14,” she said. “I’d locked them away in a little box in the back of my brain and I would never open this box but something opened it quite late in life - and I realised you only live once.” LGBT: The pilot who came out as transgender at 58” BBC 4th April 2024.
If Burton is personally uncomfortable with the actual research regarding this issue, this evidently means that there is a conflict of interest in GIRES representing this issue accurately.
In 2024, the Cass Review found that puberty blockers had been prescribed with unclear rationale and weak evidence. This is unsurprising, given GIRES were training the NHS to administer puberty blockers to a tomboy, who had seen “transgender” on YouTube:
“At first when I was little, I thought I was just a tomboy, but then on YouTube there was videos — there was a video and it said transgender. I looked at it and I realised I’ve always really wanted to be a boy, but I just couldn’t really say it… I’m hoping for the blockers to make the whole package, make me happy, and that will be that, I’ll be perfect.” “Some people might look at Kai and go “Oh ‘he’s nine or ten’ and think ‘you know the tomboy phase’ … but it’s definitely not a phase”.1
This appears to be another instance, of the well-recognised problem of men with autogynephilia, who appear to be in denial regarding their condition, advocating for medical treatments for children with “early-onset gender dysphoria”, not apparently realising that their own experience of gender dysphoria is irrelevant to what these children are experiencing.2 Given the case above, this has now resulted in child abuse.
Gendered Intelligence
In 2022, RGCP said that there was an “urgent need” for “definitive knowledge about the causes of rapidly increasing referrals” (illustrated below).

However this concern was not shared by Gendered Intelligence, who at the same time were telling children not to worry if they did not feel “trans enough” in order to participate in their youth groups:
“Our youth groups are open to all young trans people, no matter how you identify or whether you are questioning your gender. We use trans as an umbrealla [sic] term and are fully inclusive of non-binary individuals; please don’t worry about not feeling ‘trans enough’.”
This a marked departure from the DSM-4’s view of “gender identity disorder”, which sees this condition as a “profound disturbance of the individual's sense of identity with regard to maleness or femaleness. Behavior in children that merely does not fit the cultural stereotype of masculinity or femininity should not be given the diagnosis unless the full syndrome is present, including marked distress or impairment” (DSM-4 p. 536).
There is evidently a conflict of interest, as whereas the DSM-4 cautions against labeling children with this condition, it is in the interest of Gendered Intelligence for as many children as possible to apply the “trans” label to themselves, as this means more participants in its “youth groups” and more funding. This is not a small industry: in 2024, Gendered Intelligence had an expenditure of nearly £1,7 million.
In 2022, I contacted Gendered Intelligence, similar to how I contacted GIRES, asking them to cover the causes of cross-sex identification as they appear in the DSM-5, including autogynephilia. They similarly refused to do so: “We are under no obligation to reference additional material” (paragraph 85 CRM:0467599).
If Gendered Intelligence had referenced autogynephilia, then this may have resulted in fewer children, especially girls, thinking that “being trans” would apply to themselves. This would no doubt result in Gendered Intelligence being a far smaller charity than it is today.
Indeed, I do not see that Gendered Intelligence needs to exist at all; children simply do not need a social club based around presenting them with parts of the DSM-5 taken out of context, for a condition that is mostly connected to an odd male paraphilia.
In 2024, I made another complaint to Gendered Intelligence, regarding their content that made claims regarding puberty blockers, which the Cass Review showed was unsupported by evidence. Gendered Intelligence disagreed with me, yet silently deleted their content for a “redesign”.
It is arguable that Gendered Intelligence promoting puberty blockers to children without evidence, whilst keeping children and parents in the dark regarding autogynephilia, is, again, child abuse, and against the principal of informed consent.
There is a long-running issue in that the Charity Commission do not adequately regulate charities making misleading medical health claims,3 and this issue is evidently a perfect storm.
Patient groups
The RCGP says that it has consulted “patient groups”, but seems to be unaware of the fact that there is a conflict of interest in patients, especially males, in wanting to talk honestly about the actual cause of “gender dysphoria”, as they appear in the DSM-5, namely, as something that mostly only males historically experienced, and something that is connected to having an atypical sexuality / sexual orientation.
This can be seen in media accounts of autogynephilia, where individuals with autogynephilia present, or have their condition presented, solely under the guise of having a “mismatched” “gender identity” or as the RCGP now writes, having an “incongruent gender”.
Autogynephilia and “stuff fetishism”
Autogynephilia is nonetheless easy to recognise, as it clusters with specific other paraphilia, namely masochism and “stuff fetishism”, as Blanchard observed:
“Some paraphilias definitely cluster: autogynephilia and masochism, for example, and autogynephilia, masochism and what we might call “stuff fetishism”: fetishism for particular materials, like leather, silk, rubber… it’s not completely at random…”
The clustering between “stuff fetishism” and autogynephilia can be observed in the Guardian article below: the fascination with the “silky nightgown” and “wear[ing] tights under her [sic] school trousers, enjoying how they felt against her skin”:

“Hannah crept into their bedroom and tentatively opened a drawer. She took out a silky nightgown and shrugged it on, feeling the instant, giddy rush of something she would later learn to call “gender euphoria”, though it was tempered by fear that someone would walk in. As if on cue, her mother returned from work unexpectedly and caught Hannah in the act… At secondary school, she would wear tights under her school trousers, enjoying how they felt against her skin.” (‘In the game, I knew myself as Hannah’: the trans gamers finding freedom on Roblox’, Tom Faber The Guardian 24th April 2021).
The clustering between autogynephilia and “stuff fetishism” can again be observed below. In this case, Abigail Thorn’s apparent autogynephilia clusters with a preference for wearing rubber:

“Abigail Thorn: ‘I came out as trans and made headlines’”. (BBC, 3rd April 2021).

Abigail Thorn. “Transhumanism: ‘The World's Most Dangerous Idea’” Philosophy Tube (Youtube channel).
Autogynephilia and pseudobisexuality
Another phenomenon that Blanchard described, which makes autogynephilia easy to recognise is “pseudobisexuality”.4
This is not true bisexuality, as in being attracted to both men and women, but rather arousal by the thought of being a woman, with a man functioning as a “prop”, to further the conceit of being a woman. Speaking as a someone who has autogynephilia, it is not possible to understand this phenomenon, if one does not have experience of autogynephilia; it is an unusual aspect of an unusual paraphilia.
This “(pseudo)bisexuality is a common feature in media accounts of being “transgender” e.g.
“That summer Alice came downstairs from her bedroom wearing a dress for the first time — a floral item that seemed to make her giddy with happiness… Alice began dressing as a girl routinely, spoke openly about her bisexuality, and included her parents in the decision-making process to change her name after 17 years of living with a boy’s name” (The Times, “I’m ashamed it took me so long to accept my transgender child”, Laura Pullman, 9th March 2025).
Autogynephilia and the “feminine essence narrative”
The personal psychological reasons for male patients with autogynephilia not wanting to describe the causes of their cross-sex identification accurately is well documented, for example, as Anne Lawrence, a self-aware autogynephilic transsexual, writes:
“We autogynephilic transsexuals want to be women; but the theory [of autogynephilia] tells us that we are not women and that we don’t even resemble women—not in the least. We would like to believe that our desire to be women springs from our need to express some internal feminine essence; but the theory tells us that we have no internal feminine essence and that our desire to be women actually springs from our paraphilic male sexuality”.
There is also a political reason for transsexuals to prefer the narrative of having a “mismatched gender identity” or now “incongruent gender”, as this is an easier conversation to have with the public. As the bioethicist Alice Dreger writes:
“The shame and derision accorded trans women like Juanita and Cher [the two male-to-female transsexual case studies in the book] doesn’t disappear just because a few scientists may be personally fine with the idea that men might become women primarily because of reasons of sexuality, not “trapped” gender identity… They wanted the whole business of Blanchard’s taxonomic division shot down. Transsexuality should appear only as the public could stomach it, as one simple story of gender, a tale of “true” females tragically born into male bodies, rescued by medical and surgical reassignment. And there should be absolutely no mention of autogynephilia ...”5
Evidently the actual causes behind “gender dysphoria” have been successfully “shot down”, and it its place, there is the “feminine essence narrative”, under the guise of having a “mismatched” “gender identity” or now “incongruent” “gender” which suggests that male-to-female transsexuals (historically being the most common) are “in some literal sense and not just in a figurative sense, women inside men's bodies”.6
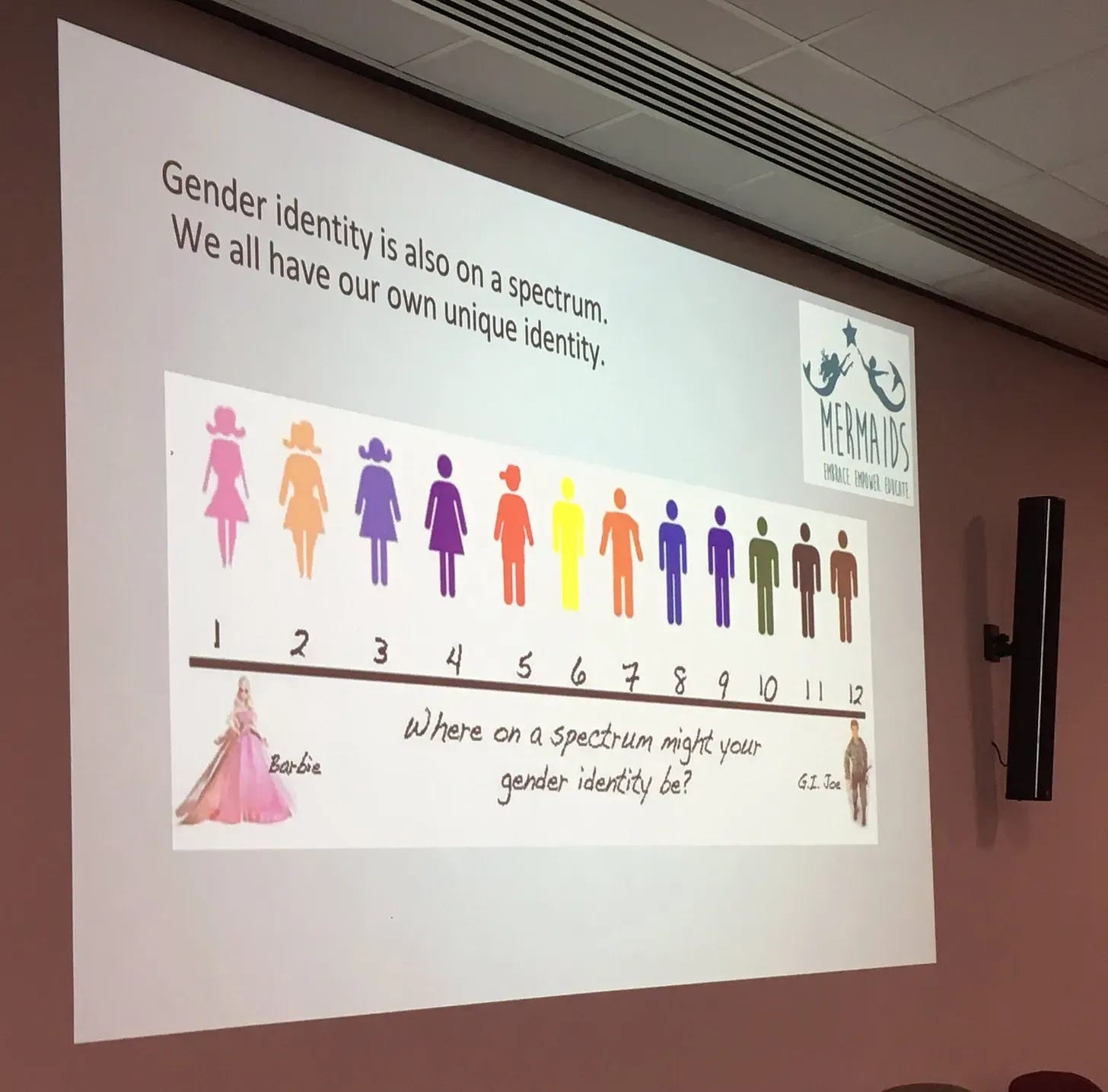
This false “feminine essence narrative” has been targeted at children for a long time, often by using crude stereotypes. For example, in Mermaid’s training material below targeted at children, Mermaids leads children to believe that if they are not a boy who is “GI Joe” or a girl who is like “Barbie”, they could have the “gender identity” or “essence” of the opposite sex.
It does not take great insight to understand that this is why there is a social contagion of primarily adolescent girls and young women who believe they have a “mismatched” “gender identity” or “incongruent gender” for not being “Barbie”:
In 2022, I complained to the Charity Commission regarding multiple charities, that the loose and misleading definitions of “gender identity” and “gender dysphoria” that charities were targeting at children was causing a social contagion, primarily amongst adolescent girls and young women, who are a cohort historically noted for suffering from misdiagnosing themselves with medical conditions. However nothing was done.
Medical malpractice
Originally, the only people who used to seek out supposed medical treatments and surgeries were men with autogynephilia, like Lili Elbe (1882 – 1931).
Now, however, the medical profession has embarked on prescribing supposed treatments and undertaking surgeries on thousands of primarily adolescent girls and young women, based on the false premise, that they have a “mismatched gender identity” or now “incongruent gender”:
“The mothers left distraught after the NHS removed their daughters’ healthy breasts because the girls said they were transgender” (Daily Mail, Sanchez Manning, 27th February 2025).
“Father’s letter begging top surgeon to cancel trans operation on ‘depressive’ 20-year-old: ‘Please don't remove my daughter's breasts ...in just one day you'll ruin her life for ever’” (Daily Mail, Sanchez Manning, 27th July 2024).
“I was desperate to be a boy and to have my breasts removed. Now I realise I was a girl all along — and this is why” (Daily Mail, Helen Carroll, 3rd April 2025).
“Revealed: More than 1,000 patients a year have trans chest surgery on the NHS” (Telegraph, Hayley Dixon, 10th February 2025).
“‘Doctors refused to let me admit my transition was a mistake. Now I want to reverse it’” (Telegraph, Sanchez Manning, 13th August 2024).
“Mum’s fury after transgender suicide teen sold hormones from illegal online clinic [GenderGP]” (Cambridge News, Anna Savva and Nicola Small, 30th June 2019).
It is necessary for the RCGP, and the wider medical profession, to stop this medical malpractice.
The RCGP can easily contribute to stopping this medical malpractice by covering the very basic information regarding the pathways gender dysphoria as they appear in the DSM-5, with a paragraph about autogynephilia, (as I do so on paragraph 10 onwards above). I have asked the RCGP to do so since 2024 (I include all previous correspondence with the RCGP below).
Yours,
Orlando Woolf.
11th January 2024
Dear RCGP,
I would like to offer feedback on your page
https://www.rcgp.org.uk/policy/rcgp-policy-areas/transgender-care
which says that “These include more definitive knowledge about the causes of rapidly increasing referrals”.
I had what is now called “gender dysphoria” as a teenage boy in the 1990s. I read research then, which has led me to be concerned with this issue today. For convenience, I have published a short referenced memo on Substack, which I'd like to share with you to hopefully convey my concerns.
The memo is: https://transpolicy.substack.com/p/trans-memo
In addition, a shorter version of my memo was recently published at
who are seeing this issue first hand.
Yours, Orlando
17th January 2024
Good evening Orlando,
Thank you for getting in touch.
Your feedback has been forwarded to the relevant department.
Kind regards,
Laiqah
Laiqah Shah
Member Services Team Leader - Admin | MDE
Royal College of General Practitioners
22nd January 2024
Dear Laiqah,
Please could I request an eventual response regarding the feedback that I have submitted, from the relevant department.
Yours, Orlando
29th January 2024
Dear Laiqah,
I was wondering if there was any update to my enquiry.
Yours, Orlando
[No reply]
20th February 2024
[Complaint]
Dear RCGP, I would like to make a complaint regarding the key definitions on your page https://www.rcgp.org.uk/policy/rcgp-policy-areas/transgender-care which suggest matters of cross-sex identification is "discomfort experienced due to a discrepancy between a person’s gender identity and their biological sex observed at birth."
I don't this as the truth, and is a narrative that is arguably causing a psychological social contagion amongst girls, who have come to believe they have the “gender identity” of the opposite sex. I have published a short referenced memo on Substack, which I'd like to share with you to hopefully convey my concerns. The memo is: https://transpolicy.substack.com/p/trans-memo
In addition, a shorter version of my memo was recently published at https://genspect.org/the-truth-about-trans who are psychologists seeing this issue first hand.
Yours, Orlando
[No reply]
30th March 2025
[Complaint]
Please could you cover the fact that there are two pathways to “gender dysphoria” in your “transgender” content.
https://www.rcgp.org.uk/representing-you/policy-areas/transgender-care
Please could you also include a paragraph on autogynephilia.
Your content misleading implies that “Gender dysphoria is ‘all one thing’”.
I am an adult with "late-onset gender dysphoria" (DSM-5 p. 455), connected to autogynephilia (DSM p. 703) "Autogynephilia is defined as a male's propensity to be sexually aroused by the thought of himself as a female".
It's a lot different from “early-onset gender dysphoria” (DSM-5 p. 455) which is connected to desistence at the onset of puberty and homosexuality.
Not distinguishing the different types of gender dysphoria, means that medical professionals cannot give the correct advice on how pathways are likely to resolve. This is an easy article that covers the different types of gender dysphoria:
https://4thwavenow.com/2017/12/07/gender-dysphoria-is-not-one-thing/
8th April 2025
Good Morning Orlando,
Thank you for submitting our complaint form.
This email is to acknowledge that your complaint was received and will respond within 20 working days in line with the College complaint procedure.
We take complaints, feedback and suggestions seriously and are working hard to respond to you.
We thank you for your time and patience with this matter.
Kind regards,
[…]
Member Services Team Leader | Member Services
Royal College of General Practitioners
25th April 2025
Dear Orlando.
We hope you're well.
Many thanks for taking the time to review our 2025 statement on the role of GPs in transgender care in detail and for sharing your comments.
We appreciate the points you have made, however with the statement now approved by our UK Council, we are unable to make any further changes at this stage. I’m sure you will understand that we aren’t able to cover all angles in the statement and have mostly sought to focus on the role of the GP specifically.
We would like to assure you that our team worked diligently with key stakeholders, to provide a balanced and informed position statement that reflects the views of frontline GPs and balances the wide range of opinions and expertise amongst our membership.
Our College will continue our work to prioritise promoting the delivery of holistic, evidence-based care to transgender patients and to influence clinical policy and practice, in this area, across the UK.
Best wishes,
RCGP Policy Team
12th May 2025
Dear RCGP,
Please could you escalate my complaint.
Your response to my complaint is inappropriate for 3 reasons:
1. The RCGP writes "Many thanks for taking the time to review our 2025 statement on the role of GPs in transgender care in detail and for sharing your comments. We appreciate the points you have made, however with the statement now approved by our UK Council, we are unable to make any further changes at this stage."
I first contacted you regarding this issue in 2024. You should have had therefore had plenty of time to include the actual pathways of “gender dysphoria” in the DSM-5. It represents a failure on your behalf that you did not.
2. The RCGP writes "I’m sure you will understand that we aren’t able to cover all angles in the statement and have mostly sought to focus on the role of the GP specifically."
I am asking you to cover the very basic pathways of "gender dysphoria" as they appear in the DSM-5, as obviously it is important for GPs to know that "early-onset gender dysphoria" mostly ceases at the onset of puberty, whereas "late-onset gender dysphoria" begins at the onset of puberty.
This is not just my view, it is the view of Blanchard, who served on the DSM-4 subcommittee for gender identity disorders and is arguably the world expert on this topic:
“It should be clear by now that “gender dysphoria” is not a precise enough term. Parents of gender dysphoric children should know which type of gender dysphoria their child has. To do so it is necessary to learn about all three of the most common types. That is, in order to understand why one’s child is Type X, it is necessary to know why s/he is not Type Y or Type Z. This is not simply academic. There are essential differences between the different types of gender dysphoria.” [1]
3. I argue that the RCGP seeks to avoid accountability for the inappropriateness of its response to my complaint, by breaking with its established convention and signing its response anonymously.
[1] https://4thwavenow.com/2017/12/07/gender-dysphoria-is-not-one-thing
Yours,
Orlando Woolf
14th May 2025
Dear Orlando,
Thank you for your most recent email which has been escalated to me.
I understand your concerns that our statement does not sufficiently cover pathways of gender dysphoria and appreciate your engagement with us on this topic over the past years.
It may be useful to differentiate between this statement which is a policy position signed off by the College’s governing Council setting out what does and does not fall within the GP role, as compared to educational materials informing GPs about the details of clinical areas such as gender dysphoria. The statement refers to a number of educational resources and this is where we would expect details of clinical pathways to be addressed. I hope this provides some further context.
The statement was developed in consultation with a wide range of RCGP members, patient groups and key stakeholder organisations. I’m afraid we are not in a position to further discuss it or any changes to it at this point, but I would like to thank you again for your careful consideration of it.
Best wishes,
Ruth
Ruth Ellenby
Head of Policy | Policy, Research and Campaigns
GIRES NHS Training video. Co-produced by NHS Surrey and Borders Partnership. Funded by NHS Health Education Kent Surrey and Sussex.

“…a number of vocal transgender activists who have histories typical of autogynephilic gender dysphorics do not hesitate to pressure parents, legislators, and clinicians for acquiescence, laws, and therapies that do not distinguish among types of gender dysphoric children. Moreover, they not infrequently claim inside knowledge based on their own experiences. Yet their experiences are irrelevant to the two types of gender dysphoria that they don’t have. And even with respect to autogynephilia, these transgender activists are nearly all in denial.” Gender dysphoria is not one thing.
“HealthSense maintains pressure on the Charity Commission regarding charities that mislead vulnerable people about health and disease.” “Abusing the public’s trust in charities”, Les Rose HealthSense issue 123.
“In their fantasies of sexual interaction with men, bisexual gender dysphorics are primarily aroused by what is, for them, the symbolic meaning of such acts, namely, the thought that they themselves are women. This type of “bisexual” orientation need not reflect an equal erotic attraction to the male and female physiques and would perhaps better characterized as pseudobisexuality.” Blanchard, R., & Steiner, B. W. (Eds.). Clinical management of gender identity disorders in children and adults. (Washington, DC: American Psychiatric Press, 1990).
Dreger, A., Galileo’s Middle Finger (Penguin, 2015) pp. 65-66.
Blanchard R. “Deconstructing the Feminine Essence Narrative”. Archives of Sexual Behavior 2008;37:434-438