
Rapid response to "Transgender identity in young people and adults recorded in UK primary care electronic patient records" by McKechnie et al.

A rapid response to “Transgender identity in young people and adults recorded in UK primary care electronic patient records: retrospective, dynamic, cohort study”.
15th January 2024
Dear Sophie Cook/BMJ Medicine,
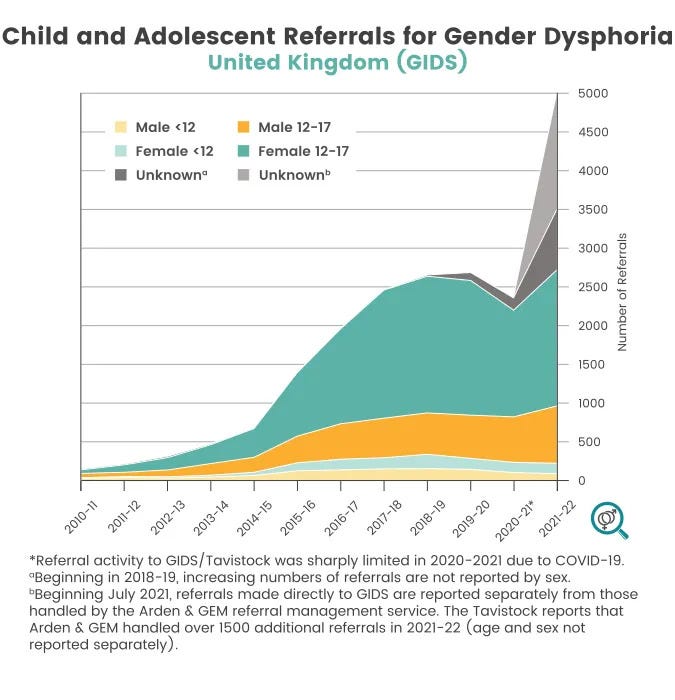
The Royal College of General Practitioners say that there is an “urgent need to expand the understanding of gender variance issues across the entire health system” they also say this “include[s] more definitive knowledge about the causes of rapidly increasing referrals”. [1]
I first contacted the BMJ’s investigations unit on the 21st July 2023 regarding the topic of rapidly increasing referrals.
I contributed my own personal experience of what today is called "gender dysphoria" along with research on this topic, and suggested the theory that the rapidly increasing referrals, primarily amongst girls, was not likely explained by this cohort having the "gender identity" of the opposite sex, and that treating them as such is to cause harm. I asked the BMJ to investigate this issue.
I was advised by Rebecca Coombes that “I'm afraid that we won't be taking this forward as a story. There are many subjects competing for investigation and we have to pick those in which we feel that we can most useful have impact.” I was advised that I could leave a rapid response to Jennifer Block’s feature “Gender dysphoria in young people is rising—and so is professional disagreement”.
I typed up a rapid response with references, [2] however it was not published.
On the publication of “Transgender identity in young people and adults” by McKechnie et al., on the 28th November 2023, I again put together a rapid response, this time with an academic who had been published in the BMJ and who I had contacted previously regarding this issue. They said they hoped that the rapid response would be published.
I submitted this rapid response on the 3rd December 2023. [3] I appreciate that this was during the lead-up to the Christmas holiday, however I was informed that rapid responses were again being considered on the 8-12th January 2024, and the rapid response remains unpublished.
In the interim period, the organisation Genspect (directed by the Irish psychotherapist Stella O'Malley), who are counsellors dealing with this issue first hand, published a shorter version of my memo highlighting my concerns on their website. [4,5].
I am attempting, as suggested by Rebecca Coombes, to contribute a rapid response with the theory that the rapid increase in referrals, primarily amongst girls, is not likely explained by the fact that they have the "gender identity" of the opposite sex, and that treating them as such is to cause harm. However my attempt to do so remains unsuccessful.
Please could you let me know if it is an issue that the rapid response was submitted anonymously. I could then try to find an academic who would put there name on it, as a report from myself.
Yours,
Orlando
[1] https://www.rcgp.org.uk/policy/rcgp-policy-areas/transgender-care
[2]
Dear Editor,
At the onset of puberty, at around 13/14 I found that I wasn’t only attracted to women, but was attracted to the concept of myself as a woman. It was a confusing phenomenon until I found research by Dr. Ray Blanchard, who described the phenomenon as "autogynephilia", from the Greek roots meaning "love of oneself as a woman". [1] I later found out, by reading the popular introduction to transsexualism "The Man who would be Queen" by Prof. J. Michael Bailey that this was one route to male transsexualism: the other being connected to femininity and homosexuality.
At this age I made the calculation that it was statistically more likely I was a male with autogynephilia, rather than a lesbian "trans woman": the ratio between hetero- and homosexual women was small; the ratio of those homosexual women supposedly “born in the wrong body” must be smaller still, leaving that idea implausible. As an adult, I find the theory of the "two types" of transsexual applies to what I observe of public life.
I have therefore been concerned for a long time that what young people are being taught about "gender identity" is not based in any of the research that I have read, and I personally feel is true. I see that the idea that someone has a "gender identity" as a reformulation of what Blanchard called the "feminine essence theory", which is the belief that "Male-to-female transsexuals are, in some literal sense and not just a figurative sense, women inside men’s bodies". [2]
I see several reasons why male transsexual activists would want to promote this belief: it is a delusion that avoids the psychological distress at considering oneself as a male with autogynephilia, [3] it makes the conversation for "trans rights" easier to have with the public, [4] and it weakens the necessity of medical safeguarding, as the issue is recast from a "gender identity disorder" that requires the oversight of mental health professionals, as understood in the DSM-4, to a matter of personal "gender identity": "Some trans people will transition (...such as changing their name or parts of their body) to make themselves feel more comfortable. This is not an illness, but just part of becoming who we are." [5]
To me, it is obvious that teaching such a loose concept of "gender identity" to children is what is causing the high referrals of children to clinics, especially girls, with "gender dysphoria". Stonewall teaches children and young people that "trans" is "An umbrella term to describe people whose gender is not the same as, or does not sit comfortably with, the sex they were assigned at birth." [6] The idea that sex is "assigned" is pseudoscientific and the idea that you might be uncomfortable with your "gender" is a near-universal part of puberty. Teenage girls are a cohort that is susceptible to socially contagious mental health issues, as Abigail Shrier writes in Irreversible Damage "One protagonist has led them all, notorious for magnifying her own psychic pain: the adolescent girl. Her distress is real. But her self-diagnosis, in each case, is flawed". [7]
I see it as irresponsible for charities, schools and non-governmental organisations to be teaching about "gender identity" to children, which I argue is a belief that misrepresents the true nature of the issue of transsexuality. Furthermore, I do not think anything regarding issues of transsexuality should be being taught indiscriminately to children. The children and young people who have difficulties, like I had, make themselves known and intervention can be provided as required, if necessary.
[1] "Early History of the Concept of Autogynephilia", Blanchard, R. Ph. D., Archives of Sexual Behavior 34(4): 439-46. September 2005.
[2] "Deconstructing the Feminine Essence Narrative", Blanchard, R. Ph. D., Archives of Sexual Behavior 37:434-438. April 2008.
[3] Lawrence, A. "Men Trapped in Men’s Bodies" (Springer, 2013). p. 202.
[4] Dreger, A. "Galileo’s Middle Finger" (Penguin: 2015) pp. 65-66.
[5] “Gender Identity (T+)” The Proud Trust https://www.theproudtrust.org/young-people/exploring-identity/gender-identity-t/
[6] "List of LGBTQ+ terms" Stonewall https://www.stonewall.org.uk/list-lgbtq-terms
[7] Shrier, A. Irreversible Damage (Regnery, 2020) p. 13.
[3]
Dear Editor,
McKechnie’s paper on “Transgender identity in young people and adults recorded in UK primary care electronic patient records: retrospective, dynamic, cohort study” [1] was interesting but coloured by ideological biases and unreliable results. The authors assert that “trans” is a matter of a supposed mismatch between one’s “gender identity” and one’s “sex assigned at birth” -- both concepts that are controversial in the literature.
Sex is not “assigned” [2] and the idea that “trans” is the result of a mismatched “gender identity” does not accord with research and my personal experience. As an adolescent in the late 1990s, I found myself questioning my sex. I searched for a reason for what I was feeling and found a synopsis of Blanchard’s research, theorising that the male cause of cross-sex identification was connected to atypical sexual orientation, namely, either homosexuality, or what he termed “autogynephilia”, meaning “love of oneself as a woman”, [3] which included the phenomenon of what Blanchard would later call “pseudobisexuality”. [4] This accurately described my experience and many others of my generation.
The authors assert that “Sexual orientation is distinct from gender identity” however it is clear to me that cross-sex identification and sexual orientation are, and can be, connected, and explains the nature of “trans” rather than the theory of “gender identity”. The assertion that a person even has a “gender identity” suggests that “Male-to-female transsexuals are, in some literal sense and not just in a figurative sense, women inside men’s bodies”. It is arguable that “gender identity” has merely replaced what Blanchard clarified as “feminine essence theory”. [5] There is no evidence that “feminine essence theory” nor its supposed reformulation as "gender identity", are the truth behind male cross-sex identification. Thus, I and many others, continue to watch with growing concern as “gender identity” theory has been taught as established dogma to children by schools, charities and non-governmental organisations.
Furthermore, it is likely that teaching children that “trans” is a matter of a mismatched “gender identity” has created a social contagion amongst girls; social contagions being a well-documented phenomenon in this cohort (and especially amongst detransitioners). [6] Abigail Shrier gives the example that in Hong Kong there had never been an epidemic of “anorexia” until their local media publicised the “Western ailment” of anorexia nervosa, which was said to have been responsible for a girl’s death. [7] The fact that the presentation of these girls is outside what researchers know about the nature of cross-sex identification, [8] further suggests the cause of their cross-sex identification is likely to be external, rather than internal.
Finally, the authors fail to comment on the value of keeping biological sex in medical records, even if patients undergo social or medical transitions. Their estimates would have been much more reliable if they could have anchored their research in the one fact (sex) from which all definitions and identity flow (whether congruent, incongruent, mismatched or not).
[1] McKechnie, DGJ, O’Nions, E., Bailey J., et. al. “Transgender identity in young people and adults recorded in UK primary care electronic patient records: retrospective, dynamic, cohort study”, BMJ Medicine 2023;2:e000499. 10.1136/bmjmed-2023-000499.
[2] “Gender-questioning children deserve better science”, Byng, R., Bewley, S., Clifford, D., McCartney, M. The Lancet 392 (2018).
[3] “The Classification and labelling of nonhomosexual gender dysphorias”, Blanchard, R., Ph. D. Archives of Sexual Behavior 18(4) 315-334 p. 323.
[4] Blanchard, R. (1990). “Gender identity disorders in adult men”, in R Blanchard & B. W. Steiner (Eds.), Clinical management of gender identity disorders in children and adults (pp. 47-76). Washington, DC: American Psychiatric Press.
[5] “Deconstructing the Feminine Essence Narrative”, Blanchard, R. Ph. D. Archives of Sexual Behavior (2008) 37:434–438.
[6] “Detransition and Desistance Among Previously Trans-Identified Young Adults”, Littman, L., O’Malley, S., Kerschner, H. et al. Archives of Sexual Behavior (2023) https://doi.org/10.1007/s10508-023-02716-1
[7] Abigail Shrier, Irreversible Damage. Regnery Publishing: 2020 p. 168.
[8] “Gender dysphoria is not one thing”, Bailey, J. M. Ph. D., Blanchard, R. Ph. D. 7 December 2017 4thWaveNow https://4thwavenow.com/2017/12/07/gender-dysphoria-is-not-one-thing/
[4] https://transpolicy.substack.com/p/trans-memo
[5] https://genspect.org/the-truth-about-trans/
23rd January 2024
Dear Orlando.
Thank you for your emails. While we aim to make decisions on rapid responses within 14 days this is an aim rather than a definitive deadline.
I'm afraid on this occasion we have decided not to publish your response online. We make clear in our T&Cs that we do require accurate author personal details and generally do not permit posting under an alias.
However, our decision on this occasion is based on the content of the response and therefore the addition of an academic author as you have previously suggested would not reverse our decision. I note that you mention in previous correspondence that in the interim another organisation has posted a version of your memo.
You can read more about our terms and conditions for rapid responses here
I must mention that all our decisions are final and I'm afraid we cannot enter into lengthy correspondence about why we have not posted a response.
Many thanks for your interest in BMJ Medicine's research article,
Best wishes,
Sophie
Dr Sophie Cook
Editor in Chief, BMJ Medicine
Head of clinical content, The BMJ
Pronouns: she/her