


Charity Commission complaint regarding Gendered Intelligence
CRM:0049630

24th September 2024
Dear Charity Commission,
I would like to make the complaint that Gendered Intelligence (1182558) is 1) conveying a misleading narrative regarding matters of cross-sex identification to children and parents 2) has encouraged children to identify as “trans” under this misleading narrative, and 3) promoted a medical treatment to children who have identified as “trans” under this misleading narrative, without medical justification.
Misleading narrative regarding matters of cross-sex identification
I am a man who has autogynephilia, which the DSM-5 defines as “Sexual arousal of a natal male associated with the idea or image of being a woman”,1 and late-onset gender dysphoria.2
Autogynephilia, and late-onset gender dysphoria, form part of the two trajectories that behind male gender dysphoria, which are described in the DSM-5, which is worth reading as a full excerpt:
“In both adolescent and adult natal males, there are two broad trajectories for development of gender dysphoria: early onset and late onset. Early-onset gender dysphoria starts in childhood and continues into adolescence and adulthood; or, there is an intermittent period in which the gender dysphoria desists and these individuals self-identify as gay or homosexual, followed by recurrence of gender dysphoria. Late-onset gender dysphoria occurs around puberty or much later in life. Some of these individuals report having had a desire to be of the other gender in childhood that was not expressed verbally to others. Others do not recall any signs of childhood gender dysphoria. For adolescent males with late-onset gender dysphoria, parents often report surprise because they did not see signs of gender dysphoria during childhood. Expressions of anatomic dysphoria are more common and salient in adolescents and adults once secondary sex characteristics have developed. Adolescent and adult natal males with early-onset gender dysphoria are almost always sexually attracted to men (androphilic). Adolescents and adults with late-onset gender dysphoria frequently engage in transvestic behavior with sexual excitement. The majority of these individuals are gynephilic or sexually attracted to other post transition natal males with late-onset gender dysphoria. A substantial percentage of adult males with late-onset gender dysphoria cohabit with or are married to natal females. After gender transition, many self-identify as lesbian. Among adult natal males with gender dysphoria, the early-onset group seeks out clinical care for hormone treatment and reassignment surgery at an earlier age than does the late-onset group. The late-onset group may have more fluctuations in the degree of gender dysphoria and be more ambivalent about and less likely satisfied after gender reassignment surgery.”3
The DSM-5 shows cross-sex identification is connected to atypical sexuality / sexual orientation, namely related to either autogynephilia, or homosexuality.
In comparison, Gendered Intelligence presents cross-sex identification as a matter of a somehow “mismatched gender identity”:
“People may use the term ‘trans’ to describe themselves if their own sense of gender (their gender identity) does not match or sit easily with the gender they were assumed to have based on the sex they were assigned at birth.”4
This narrative suggests that transsexuals are “in some literal sense and not just in a figurative sense, women inside men's bodies” (male-to-female transsexualism being historically the most common).5 This narrative is known in research as the “feminine essence narrative”, and is a fiction, which the reader can see does not represent what is written in the DSM-5 regarding matters of cross-sex identification.
I cover in my “Trans memo” (http://transpolicy.substack.com/p/trans-memo) the history and motivation that activists have in promoting this narrative, which I have shared with the Charity Commission many times.
Omitting research
In 2022, I complained to Gendered Intelligence, saying that their narrative regarding issues of cross-sex identification was misleading, and that they were omitting research that shows the cause behind cross-sex identification is related to atypical sexuality / sexual orientation, namely, autogynephilia or homosexuality.
Despite this, Gendered Intelligence chose to continue to omit this research, saying “we are under no obligation to reference additional material”.6 There appears to be no good reason why Gendered Intelligence would say this, given that medical professionals, such as Ray Blanchard, who served on the gender identity disorder subcommittee of the DSM-4, says that it is essential for parents to recognise that there are different pathways and reasons to gender dysphoria:
“Parents of gender dysphoric children should know which type of gender dysphoria their child has. To do so it is necessary to learn about all three of the most common types. That is, in order to understand why one’s child is Type X, it is necessary to know why s/he is not Type Y or Type Z. This is not simply academic. There are essential differences between the different types of gender dysphoria. If knowledge is power, then lack of knowledge is malpractice.”7
Also in 2022, I followed up my complaint with a complaint to the Charity Commission, regarding Gendered Intelligence, and other charities who are promoting the “mismatched gender identity” narrative. (CRM:0467599), to which I received the following response:
“The Commission has considered the issues raised and our assessment is that we lack the expertise and knowledge of complicated psychological and medical issues connected to gender identities to be able to form a definitive view on the issues you have raised. We note the evidence you have put forward from various professionals, but it seems to the Commission that the issues raised are matters that are unsettled and are subject to debate, interpretation, and disagreement”.8
The Charity Commission decided to take no action. I disagreed in 2022 that this was the correct decision, as I disagree with it now. If the Charity Commission’s response was that “the issues raised are matters that are unsettled and are subject to debate, interpretation, and disagreement”, this should have been a sign to the Charity Commission, that it was wrong for charities to teach children material that reflected none of this debate amongst professionals, to children who are certainly not any more capable than the Charity Commission of assessing whether the material they are being taught is true.
I followed up my complaint to the Charity Commission, by publishing an article with the charity HealthSense, which argued that charities are teaching a misleading narrative of matters of cross-sex identification to children and parents, which they are only able to do by omitting research, and that the Charity Commission provides no recourse to the public to challenge this:
https://www.healthsense-uk.org/publications/newsletter/newsletter-127/420-127-orlando.html
I note, that through my efforts, any parents working for the Charity Commission will now have an accurate understanding of the research behind cross-sex identification, so if any of their children suddenly present as “trans”, then the parents of the Charity Commission will be well informed of the correct routes to take, and can discount the false narrative that their child has a “mismatched gender identity” of the opposite sex.
However by deciding to take no action regarding my complaint, the Charity Commission does not afford the parents of the general public a similar opportunity to be informed about what is happening if their child suddenly identifies as “trans”.
Encouraging children to identify as “trans” under this misleading narrative
In 2022, the Royal College of General Practitioners (RGCP) said that there was an “urgent need” for “definitive knowledge about the causes of rapidly increasing referrals”.9
Statistics show, that the bulk of referrals were now being made up of girls and young women (illustrated on the next page).
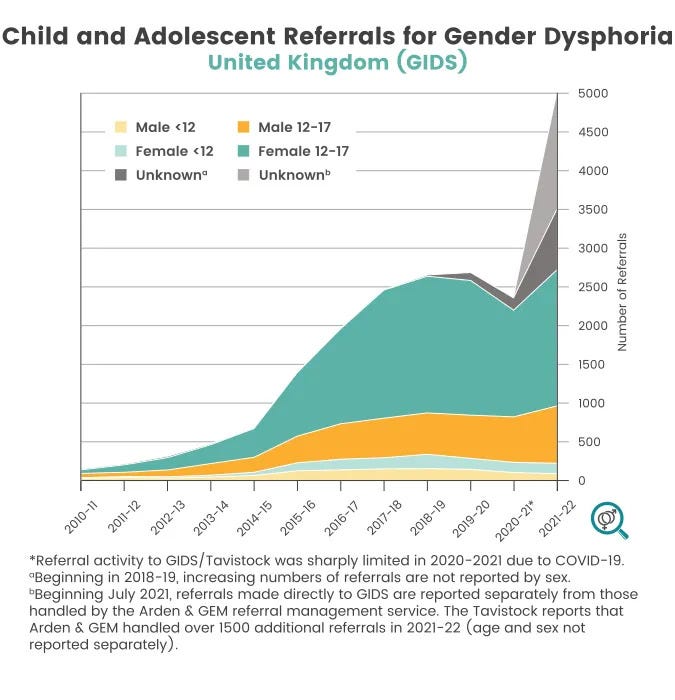
This cohort has, historically, not be represented amongst transsexuals, but is a cohort that is known to suffer from mental health social contagions,10 making it more than likely that increase in referrals is not through a new social acceptance of a pre-existing endogenous condition, but rather from girls and young women misdiagnosing themselves with a “mismatched gender identity”.
At the same time as the RGCP found increasing referral statistics a matter of concern, this was not a concern shared by Gendered Intelligence, who told children not worry that they don’t feel “trans enough”, encouraging children to misdiagnose themselves with a condition they were never historically likely to suffer from, in order to attend their “youth groups”:
“Our youth groups are open to all young trans people, no matter how you identify or whether you are questioning your gender. We use trans as an umbrealla [sic] term and are fully inclusive of non-binary individuals; please don’t worry about not feeling ‘trans enough’.”11
Promoted a medical treatment to “trans” children without evidence
So far, therefore, Gendered Intelligence have encouraged children to identify as “trans”, omitted research that suggests they might not be “trans”, and now, the conclusions of the Cass Review show that Gendered Intelligence have been promoting a supposed medical treatment, namely puberty blockers, to children without medical evidence. The Cass Review found that, regarding puberty blockers:
“The rationale for early puberty suppression remains unclear, with weak evidence regarding the impact on gender dysphoria, mental or psychosocial health. The effect on cognitive and psychosexual development remains unknown.”12
In comparison, Gendered Intelligence, in its “A Guide for Young Trans People”, claimed:
“puberty delaying treatment (PDTs) or ‘blockers’, and hormone replacement therapy (HRT). PDTs are used to delay the onset of the changes associated with puberty to allow time for exploration of gender identity”.13
I complained to Gendered Intelligence, who initially stood by their content, but shortly thereafter removed the “guide” from their website for a “redesign”.14
I made another complaint to the Charity Commission, (CRM:0049558) saying that despite the Cass Review, Gendered Intelligence, Stonewall and the Gender Identity Research and Education Society (GIRES) continue to make unfounded claims regarding puberty blockers.15
I received a message back from the Charity Commission on the 6th August 2024, saying:
“As you may be aware, the Independent Review of Gender Identity Services for Children and Young People (‘The Cass Review’) commissioned by NHS England and NHS Improvement in Autumn 2020 published its final report in April 2024. The Cass Review set out its recommendations on a range of issues which affect children and young people who are questioning their gender identity or experiencing gender dysphoria. This has resulted in changes to NHS guidelines, in particular with regard to the clinical approach to care and support. It is not for the Commission to determine whether information issued and published by charities is correct. We have decided that on this occasion the best way forward is to provide the trustees with regulatory advice and guidance about ensuring that they have regard to the findings, conclusions and recommendations of the Cass Review and ensuring that they have reviewed their charity’s literature, website and guidance in light of them.”
It is, however, the responsibility of the Charity Commission to take enforcement action when there is malpractice or misconduct regarding charities. It is under the remit of the Charity Commission to issue warnings to charities that are promoting a supposed medical treatment to children, which has now been explicitly been found without rationale or clear evidence by the NHS. This is misconduct on the behalf of charities, and is something that poses a serious risk to beneficiaries, and particularly vulnerable beneficiaries, namely children who for whatever reason are distressed regarding their sex, and are being told that puberty blockers will be a remedy for their distress, without medical evidence.
I note that as of today, 24th September 2024, any message that the Charity Commission may have sent to Stonewall and the Gender Identity Research and Education Society (GIRES) has been ignored, as these charities continue to promote puberty blockers to children and parents:
For example, Stonewall continue to promote puberty blockers on their website:
“In the UK, after assessment, this can involve being prescribed puberty blockers. This non-permanent treatment gives young people time and space to work out what is right for them, without the distress of the heightened dysphoria that puberty can bring on. It can also help those who know for sure that they do not want to experience the puberty that will occur for them without intervention.”16
As do GIRES:
“Gender dysphoria in children & young people: Gender discomfort may emerge in early childhood or adolescence and continue into adulthood. Stress is increased during puberty with the development of unwanted changes to the body. Some young people access safe, reversible intervention to interrupt puberty (hormone blockers), allowing more time to confirm how they wish to live in their adult lives.”17
I note that in 2014, the Rt Hon Margaret Hodge MP said that the Charity Commission was not fit for purpose:
“The Commission has placed insufficient emphasis on the monitoring and investigation of charities relying mainly on receiving information from others, rather than actively generating its own information and intelligence to identify risks in individual charities. The Commission is too willing to accept what charities tell it, without verifying or challenging the claims made, and it does not appropriately prioritise its limited resources to investigate the most serious cases of potential abuse of charitable status.”18
I am in agreement with this assessment today, a decade later. The Charity Commission had an opportunity to deal with charities promoting a misleading narrative regarding issues of cross-sex identification in 2022, however did not.
The Charity Commission similarly has an opportunity to use the information from the Cass Review to issue warnings to charities that continue to promote a medical treatment to children without medical justification, however, again, does not.19
I find it extraordinary that Gendered Intelligence remains a charity, despite the fact that they continue to encourage children to identify as “trans” under the misleading “mismatched gender identity”, “feminine essence” narrative; have omitted research to serve this narrative, then have been found to have been promoting a medical treatment to children, which cannot be justified by medical research.
Yours,
Orlando
DSM-5 p. 818
DSM-5 p. 703 “autogynephilia increases the likelihood of gender dysphoria...”
DSM-5 p. 455-6
Blanchard R. “Deconstructing the Feminine Essence Narrative”. Archives of Sexual Behavior 2008;37:434-438
Abigail Shrier Irreversible Damage p. 254.

